

News you can use!
Welcome to Monday, folks. In this video, Dr Ivo talks you through The Gait Guys modification of the FIM (foot intrinsic muscle) or what is sometimes called the “short foot” exercise.
Now go do it!
News you can use!
Welcome to Monday, folks. In this video, Dr Ivo talks you through The Gait Guys modification of the FIM (foot intrinsic muscle) or what is sometimes called the “short foot” exercise.
Now go do it!
Gait and Climbing: Part 1
Lucid Dreaming is the name of a rock in the Buttermilks of Bishop, California. This is no ordinary rock. It is a V15. Summiting this rock is basically only 3 moves off of 3 holds, from your fingertips. The remainder of the climb is sliced bread. If you can do the 3, you can get to the top. The problem is, only a handful of people in the world can do it. How hard can this be, after all you start sitting down.
Strength, stability, mobility, endurance, skill, experience, movement patterns … . it is all here, today, on The Gait Guys blog.
Author: Dr. Shawn Allen
There are things that other people can do in life that rattle your brain. These are tasks that these individuals make look fairly simple, but in actuality are nearly impossible to the average person. The honest fact is that many of us could do many of these things to a degree if we would dedicate a portion of our day to building the engine to perform these tasks, but the truth is that many of us would rather sit down and be entertained than get up and struggle.
Here on The Gait Guys blog, bipedal and quadrupedal gait has been discussed for over 5 years. Discussions have gone deep into the strange quadrupedal gait of Uner Tan Syndrome and have delved into the critical neurology behind CPG’s (Central Pattern Generators) which are neural networks that produce rhythmic patterned outputs. We have gone on and on about arm swing and how they are coordinated with the legs and opposite limb in a strategic fashion during walking running gaits.
Today I will look briefly at the interconnected arm and leg function in a high functioning human arguably one of the best new hot shots in climbing, Alex Megos. This year the German, as seen in this video link today, managed to summit Lucid Dreaming, a V15 in the Buttermilks of Bishop, California. Hell, you can say that this is just a big boulder, but there are not many V15s in the world like this one. Only a few of the very best in the world have even tried this rock, and you can count even fewer who have reached the summit. So, what does V15 mean to you? “virtually impossible” just about sums it up. Watch the video, this V15 starts from a “sit-start”, many folks wouldn’t even get their butts off the ground to complete the first move, that is how hard this is. Watch the video, if this does not cramp your brain, you perhaps you don’t have one.
Are there possible neurologic differences in climbers such as Megos as compared to other quadruped species? Primarily, there is suspect of an existing shift in the central pattern generators because of the extraordinary demand on pseudo-quadrupedal gait of climbing because of the demand on the upper limbs and their motorneuron pools to mobilize the organism up the mountain. We know these quadrupedal circuits exist. In 2005 Shapiro and Raichien wrote “the present work showed that human QL(quadrupedal locomotion) may spontaneously occur in humans with an unimpaired brain, probably using the ancestral locomotor networks for the diagonal sequence preserved for about the last 400 million years.”
As we all know, the interlimb coordination in climbing and crawling biomechanics shares similar features to other quadrupeds, both primate and non-primate, because of similarities in our central pattern generators (CPG’s). New research has however determined that the spaciotemportal patterns of spinal cord activity that helps to mediate and coordinate arm and leg function both centrally, and on a cord mediated level, significantly differ between the quadruped and bipedal gaits. In correlation to climbers such as Megos however, we need to keep in mind that the quadrupedal demands of a climber (vertical) vastly differ in some respects to those of a non-vertical quadrupedal gait such as in primates, in those with Uner Tan Syndrome and during our “bear crawl” challenges in our gyms. This should be obvious to the observer in the difference in quadrupedal “push-pull” that a climber uses and the center-of-mass (COM) differences. To be more specific, a climber must reduce fall risk by attempting to keep the COM within the 4 limbs while remaining close to the same surface plane as the hands and feet (mountain) while a primate, human or Uner Tan person will choose to “tent up” the pelvis and spine from the surface of contact which narrows the spreading of the 4 contact points. Naturally, this “tenting up” can be reduced, but the exercise becomes infinitely more difficult, to the point that most cannot quadrupedally ambulate more than a very short distance. I will discuss this concept in Part 2 of this series on climbing. If you study childhood development and crawling patterns, you need to be familiar with UTS (search our blog, save yourself the time), the flaws in the neurology behind the "Bird Dog” rehab pattern, and crawling mechanics … and of course, study climbers.
Some research has determined is that in quadrupeds the lower limbs displayed reduced orientation yet increased ranges of kinematic coordination in alternative patterns such as diagonal and lateral coordination. This was clearly different to the typical kinematics that are employed in upright bipedal locomotion. Furthermore, in skilled mountain climbers, these lateral and diagonal patterns are clearly more developed than in study controls largely due to repeated challenges and subsequent adaptive changes to these lateral and diagonal patterns. What this seems to suggest is that there is a different demand and tax on the CPG’s and cord mediated neuromechanics moving from bipedal to quadrupedal locomotion. There seemed to be both advantages and disadvantages to both locomotion styles. Moving towards a more upright bipedal style of locomotion shows an increase in the lower spine (sacral motor pool) activity because of the increased and different demands on the musculature however at the potential cost to losing some of the skills and advantages of the lateral and diagonal quadrupedal skills. Naturally, different CPG reorganization is necessary moving towards bipedalism because of these different weight bearing demands on the lower limbs but also due to the change from weight bearing upper limbs to more mobile upper limbs free to not only optimize the speed of bipedalism but also to enable the function of carrying objects during locomotion.
The take home seems to suggest that gait retraining is necessary as is the development of proper early crawling and progressive quadruped locomotor patterns. Both will tax different motor pools within the spine and thus different central pattern generators (CPG). A orchestration of both seems to possibly offer the highest rewards and thus not only should crawling be a part of rehab and training but so should forward, lateral and diagonal pattern quadrupedal movements, on varying inclines for optimal benefits. Certainly I need to do more work on this topic, the research is out there, but correlating the quad and bipedal is limited. I will keep you posted. Be sure to read my 3 part series on Uner Tan Syndrome, here on The Gait Guys blog. Some of today’s blog is rehash of my older writings, naturally I am setting the stage for “Part 2″ of Climbing.
- Dr. Shawn Allen
References:
Shapiro L. J., Raichien D. A. (2005). Lateral sequence walking in infant papio cynocephalus: implications for the evolution of diagonal sequence walking in primates. Am. J. Phys. Anthropol.126, 205–213 10.1002/ajpa.20049
Scand J Med Sci Sports. 2011 Oct;21(5):688-99. Idiosyncratic control of the center of mass in expert climbers. Zampagni ML , Brigadoi S, Schena F, Tosi P, Ivanenko YP
J Neurophysiol. 2012 Jan;107(1):114-25. Features of hand-foot crawling behavior in human adults. Maclellan MJ, Ivanenko YP, Cappellini G, Sylos Labini F, Lacquaniti F.
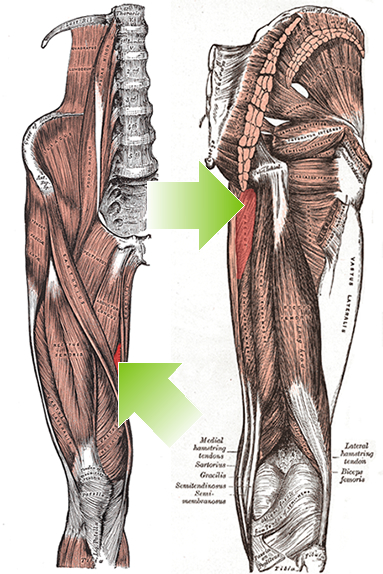
Thoughts on the adductor grouping to ponder.
I found this while prepping for the dry needling course I am teaching this weekend and thought you may enjoy it. Though the primary actions of the addcutors are well established, secondary actions (whether they are acually internal or external rotators) remains to be elucidated.
Here is a nice abstract that supports the dynamic function of them as external rotators (eccentrically) during gait.
“Anatomical texts agree on most muscle actions, with a notable exception being the action of the adductors of the hip in the transverse plane. Some texts list an action of the adductor brevis (AB), adductor longus (AL), and/or adductor magnus (AM) as internal rotation, whereas others list an action of external rotation. The purpose of this article is to present a functional model in support of the action of external rotation. Transverse plane motion of the femur at the hip during normal gait is driven by subtalar joint motion during the loading response, terminal stance, and preswing phases. During the loading response, the subtalar joint pronates, and the talus adducts. This talar adduction results in the lower leg, and subsequently the femur, internally rotating. During terminal stance and preswing, the opposite occurs; the subtalar joint supinates as the talus abducts in response to forces generated from the lower extremity and in the forefoot. Electromyographic (EMG) studies indicate varied activity in the AB, AL, and AM during the loading response, terminal stance, and preswing phases of the gait cycle. A careful analysis of EMG activity and kinematics during gait suggests that, in the transverse plane, the adductors may be eccentrically controlling internal rotation of the femur at the hip during the loading response, rather than the previously reported role as concentric internal rotators. In addition, these muscles may also concentrically produce external rotation of the femur at the hip during terminal stance and preswing. Physical therapists should consider this important function of the hip adductors during gait when evaluating a patient and designing an intervention program. Anatomical texts should consider listing the concentric action of external rotation of the femur at the hip as one action of the AB, AL, and AM, particularly when starting from the anatomic position.”
Leighton RD. A functional model to describe the action of the adductor muscles at the hip in the transverse plane.Physiother Theory Pract. 2006 Nov;22(5):251-62.Leighton RD. A functional model to describe the action of the adductor muscles at the hip in the transverse plane.Physiother Theory Pract. 2006 Nov;22(5):251-62.
The Minimalist Shoe Index, Pincer toe nails, toe problems, anteromeniscofemoral impingement syndrome and much more on today’s show !
A. Link to our server: http://traffic.libsyn.com/thegaitguys/pod_96f.mp3
Direct Download: http://thegaitguys.libsyn.com/podcast-96
Other Gait Guys stuff
B. iTunes link:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138
C. Gait Guys online /download store (National Shoe Fit Certification & more !)
http://store.payloadz.com/results/results.aspx?m=80204
D. other web based Gait Guys lectures:
Monthly lectures at : www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
-Our Book: Pedographs and Gait Analysis and Clinical Case Studies
Electronic copies available here:
-Amazon/Kindle:
http://www.amazon.com/Pedographs-Gait-Analysis-Clinical-Studies-ebook/dp/B00AC18M3E
-Barnes and Noble / Nook Reader:
http://www.barnesandnoble.com/w/pedographs-and-gait-analysis-ivo-waerlop-and-shawn-allen/1112754833?ean=9781466953895
https://itunes.apple.com/us/book/pedographs-and-gait-analysis/id554516085?mt=11
-Hardcopy available from our publisher:
http://bookstore.trafford.com/Products/SKU-000155825/Pedographs-and-Gait-Analysis.aspx
Show notes:
1. New Cameras In Japan Can Detect Drunks At Train Stations
http://www.popsci.com/cameras-japan-detect-drunks-train-stations
2. It takes a lot of nerve: Scientists make cells to aid peripheral nerve repair
http://www.medicalnewstoday.com/releases/297854.php
-Scientists at the University of Newcastle, UK, have used a combination of small molecules to turn cells isolated from human skin into Schwann cells
3. The Minimalist Shoe Definition study
http://www.jfootankleres.com/content/8/1/42
A consensus definition and rating scale for minimalist shoes
Jean-Francois Esculier123, Blaise Dubois13, Clermont E. Dionne14, Jean Leblond2 andJean-Sébastien Roy12* http://www.jfootankleres.com/content/8/1/42
modified Delphi study, 42 experts from 11 countries
http://www.jfootankleres.com/content/supplementary/s13047-015-0094-5-s1.pdf
-Results
The following definition of minimalist shoes was agreed upon by 95 % of participants: “Footwear providing minimal interference with the natural movement of the foot due to its high flexibility, low heel to toe drop, weight and stack height, and the absence of motion control and stability devices”. Characteristics to be included in MI were weight, flexibility, heel to toe drop, stack height and motion control/stability devices, each subscale carrying equal weighing (20 %) on final score.
4. CASE:
Ivo: broken toe, prioprioception
this: http://www.ncbi.nlm.nih.gov/pubmed/2245598
and this http://www.ncbi.nlm.nih.gov/pubmed/19955289
5. CASE: anterior meniscofemoral impingment syndrome
http://tmblr.co/ZrRYjx1d8503W
http://thegaitguys.tumblr.com/post/17713779565/anterior-knee-pain-in-a-young-marathon-hopeful
6. Pincer Toe nails:
http://thegaitguys.tumblr.com/post/127638788139/pincher-nails-who-knew-note-there-are-two–
As this study suggests, it has been difficult to find studies that establish a clear connection between gait stability and gait speed. One can easily assume that slowing down increases stability, we do it on slippery surfaces, we do it when a joint is painful, even the elderly do it naturally everyday. Walking speed, step length, step frequency, step width, local dynamic stability , and margins of stability were measured in this study below. It was found that the subjects did not change walking speed in response to the balance perturbations rather they made shorter, faster, and wider steps with increasing perturbation intensity. They became locally less stable in response to the perturbations but increased their margins of stability in medio-lateral and backward direction.
So what did they conclude ? Here are their words,“In conclusion, not a lower walking speed, but a combination of decreased step length and increased step frequency and step width seems to be the strategy of choice to cope with medio-lateral balance perturbations, which increases Margins of Stability (MoS) and thus decreases the risk of falling.”
It is my assumption, and this just seems logical, that if the perturbations were to continue constantly, that one would slow the gait speed to reduce the need for these shorter, faster and wider steps.
Dr. Shawn Allen
http://www.ncbi.nlm.nih.gov/pubmed/22464635
Gait Posture. 2012 Jun;36(2):260-4. doi: 10.1016/j.gaitpost.2012.03.005. Epub 2012 Mar 29.Speeding up or slowing down?: Gait adaptations to preserve gait stability in response to balance perturbations.Hak L1, Houdijk H, Steenbrink F, Mert A, van der Wurff P, Beek PJ, van Dieën JH.
Unique adaptations to arm swing challenges: the one armed runner. Welcome to Luke Ericson, an amazing athlete and man.
Written By Dr. Shawn Allen
Human gait is cyclical. For the most part, when one limb is engaged on the ground (stance phase), the other is in swing phase. Before I continue, you should recall that there is a brief double limb support phase in walking gait, that which is absent in running gait. Also, I wish to remind you of our time hammered principle that when the foot is on the ground the glutes are heavily in charge, and when the foot is in the air, the abdominals are heavily in charge.
For one to move cleanly and efficiently one would assume that the best way to do that would be to ensure that the lower 2 limbs are capable of doing the exact same things, with the same timing, same skill, same endurance and same strength. This goes for the upper 2 limbs as well, and then of course the synchronizing of the 4 in a cohesive effort. For this clean seamless motor function to occur, one must assume that there would be no injuries that had left a remnant mark on one limb thus encouraging a necessary compensation pattern in that limb (and one that would then have to be negotiated with the opposite limb as well as the contralateral upper or lower limb).
Removing a considerable mass of tissue anywhere in the body is going to change the symmetry of the body and require compensations. One can clearly see the effects of this on this athletes body in the video above. He even eludes to the fact that he has a scoliosis, no surprise there. There is such an unequal mass distribution that there is little way the spine had any chance to remain straight. Not only is this going to change symmetry from a static postural perspective (bulk, weight, fascial plane changes, strength etc) but it will change dynamic postural control, mobility and stability as well as dynamic spinal kinematics. I have talked about this previously in a blog piece I wrote on post-mastectomy clients display changes in spatiotemporal gait parameter such as step length and gait velocity.
-mastectomy post: http://tmblr.co/ZrRYjx1XB8RhO
If you have been with The Gait Guys for more than a year you will know that impairing an arm swing will show altered biomechanics in the opposite lower limb (and furthermore, if you alter one lower limb, you begin a process of altering the biomechanical function and rhythmicity of the opposite leg as well.) You can search the blog for “arm swing part 1 and part 2″ for those dialogues.
Arm swing impairment is a real issue and it is one that is typically far overlooked and misrepresented. The intrinsic effects of altering the body through subtraction of tissue are not all that dissimilar to extrinsic changes into the system from things like walking with a handbag/briefcase, walking with a shoulder bag, walking and running with an ipod or water bottle in one hand. And do not forget other intrinsic problems that affect spinal symmetry, for example consider the changes on the system from scoliosis as in this case. It can cycle back on its own feedback loop into the system, either consciously or unconsciously altering arm swing and thus global body kinematics.
There is a reason that in my practice I often assess and treat contralateral upper and lower limbs as well as to address remnants from old injuries whether they are symptomatic or not. It all comes together for the organism as a concerted effort in optimal locomotion.
Here on TGG, and in dialogues with Ivo on our podcast, I have long talked about phasic and anti-phasic motions of the arms and shoulder-pelvic blocks during gait and locomotion/sport activity. I have written several times about the effects of spine pain and how spine pain clients reduce the anti-phasic rotational (axial) nature of the shoulder girdle and pelvic girdle. In the video above, you can see anything but anti-phasic gait, to be clear, this is a classic representation of a phasic gait. The shoulder block and the pelvic block show little if any counter rotation, they are linked together which is not normal gait. Furthermore, if you look carefully, the timing of the right arm swing is variable and cyclically changing in its timing with the left leg. Look carefully, you will see the cyclical success and failure at the beginning of the video. This is pathologic gait, he must be constantly fighting frontal plane sway because there is no axial anti-phasic motion. He is also constantly fighting the unidirectional rotation that the absence of an entire limb and limb girdle is presenting, you can see him struggle with this if you have looked at enough gait samplings. There is essentially frozen torso movements. Want to see more of our work on arm swing ? search the gait guys blog.
There is so much more here to discuss, so I will likely return to this video another time to delve into those other things on my mind. Luke is an amazing athlete, he gets much respect from me.
I hope this dialogue helps you to get a deeper grip on gait and gait problems. I have written many articles on the topics of arm swing, phasic and anti-phasic gait, central pattern generators. The are all archived here on the blog. I try to write a new original thought-process article each week for the blog amongst the other “aggregator” type stuff we share from other folks social media. My weekly article serves to go deeper into things, sometimes they are well referenced and in this case, I am basing today’s discussion on the referenced work in the other pieces I have written on arm swing, phasic and anti-phasic gait, central pattern generators etc. So please do your readings there before we begin debate or dialogue, which i always welcome !
Dr. Shawn Allen
Dr Ivo demonstrating a dry needling technique for the abductor hallucis brevis

!!!! Don’t deny it, you are curious, and so are we smile emoticon We are easily distracted by bright shiny things and this one sure has the “wait, what the #$%&@ was that !” factor.
Inspired by the oversized tires found on “Fat Bikes”, the Michelin® Wild Gripper outsole welcome to the UnderArmor Fat Tire GTX Trail shoe.
2015 “Outside Gear Of The Show” Winner.
Could be a disaster or an ingenious idea. We hope to get a pair to review and let our brethren here know.
https://www.underarmour.com/…/mens-ua-fat-tire-g…/pid1262064
Chronic achilles-problem clients, slow or non-responders ?
This study suggested that , “Degenerative arthritic changes of the posterior calcaneal wall cartilage characterize patients with IAT (insertional achilles tendonotpathy) and the severity of such changes is directly correlated to the degree of functional impairment.”
Read up… . .
We have a strong show for you today. Ankle instability from a neurologic perspective, shoe wear, head tilt and the neurologic and functional complications… we also talk about Efferent Copy and motor learning.
A. Link to our server:
http://traffic.libsyn.com/thegaitguys/pod_95final.mp3
Direct Download: http://thegaitguys.libsyn.com/pod-95
-Other Gait Guys stuff
B. iTunes link:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138
C. Gait Guys online /download store (National Shoe Fit Certification & more !)
http://store.payloadz.com/results/results.aspx?m=80204
D. other web based Gait Guys lectures:
Monthly lectures at : www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
-Our Book: Pedographs and Gait Analysis and Clinical Case Studies
Electronic copies available here:
-Amazon/Kindle:
http://www.amazon.com/Pedographs-Gait-Analysis-Clinical-Studies-ebook/dp/B00AC18M3E
-Barnes and Noble / Nook Reader:
http://www.barnesandnoble.com/w/pedographs-and-gait-analysis-ivo-waerlop-and-shawn-allen/1112754833?ean=9781466953895
https://itunes.apple.com/us/book/pedographs-and-gait-analysis/id554516085?mt=11
-Hardcopy available from our publisher:
http://bookstore.trafford.com/Products/SKU-000155825/Pedographs-and-Gait-Analysis.aspx
Show notes:
Human exoskeletons: The Ekso
http://www.thedailybeast.com/articles/2015/08/03/the-mechanical-exoskeleton-shaping-the-future-of-health-care.html
Ankle muscle strength influence on muscle activation during dynamic and static ankle training modalities
http://www.tandfonline.com/doi/abs/10.1080/02640414.2015.1072640?rfr_id=ori%3Arid%3Acrossref.org&url_ver=Z39.88-2003&rfr_dat=cr_pub%3Dpubmed&#.VcYWR-1VhBc
Chronic ankle instability:
http://tmblr.co/ZrRYjx1akudcm
http://tmblr.co/ZrRYjx1ah6ThV
http://thegaitguys.tumblr.com/post/68785250796/just-because-a-muscle-tests-weak-doesnt-mean-it
http://thegaitguys.tumblr.com/post/117109093439/last-week-we-ran-an-archived-piece-named-just
the future of footwear and orthotics ?
http://lermagazine.com/special-section/conference-coverage/the-future-of-footwear-and-orthoses-is-here-now-what
squats- head posture-gait vision-gravity
http://thegaitguys.tumblr.com/search/vision
Music: brain rhythm
http://www.kurzweilai.net/the-brains-got-rhythm
Last year we were two of 42 experts worldwide from 11 countries asked to participate and offer our thoughts in an investigation whose goal it was to come up with a rating scale and definition for minimalist shoes.
Here is that study:
A consensus definition and rating scale for minimalist shoes. Jean-Francois Esculier123, Blaise Dubois13, Clermont E. Dionne14, Jean Leblond2 andJean-Sébastien Roy. Journal of Foot and Ankle Research 2015, 8:42
here is a link for that study: http://www.jfootankleres.com/content/8/1/42
This study was performed by very capable and respected folks so you should pay attention.
Here was their background statement:
“While minimalist running shoes may have an influence on running biomechanics and on the incidence of overuse injuries, the term “minimalist” is currently used without standardisation. The objectives of this study were to reach a consensus on a standard definition of minimalist running shoes, and to develop and validate a rating scale that could be used to determine the degree of minimalism of running shoes, the Minimalist Index (MI).”
We might not do the study justice if we paraphrased the conclusions, so here they are as written,
“The following definition of minimalist shoes was agreed upon by 95 % of participants: “Footwear providing minimal interference with the natural movement of the foot due to its high flexibility, low heel to toe drop, weight and stack height, and the absence of motion control and stability devices”. Characteristics to be included in MI were weight, flexibility, heel to toe drop, stack height and motion control/stability devices, each subscale carrying equal weighing (20 %) on final score.”
So why is this study important ? Well, it creates a common term, a standardized definition, we can all agree upon which is paramount for clear communication amongst professionals in fields (shoe fitters, shoe fabricators, clinicians and researchers) who are dealing with these types of shoes. This study also create a rating scale that will be meaningful to all users in all related fields, again allowing a common dialogue with standardized meaning. From this study they wisely recommended “the shoe industry use such standardised ratings to orientate the running community when selecting their running shoes”.
This is an important study, it should be part of your knowledge and vocabulary. You should familiarize yourself to the rating scale.
Shawn and Ivo, the gait guys
Gait and Concussions.
The big movie trailer just came out yesterday, click on the link above to watch the trailer for “Concussion” with Will Smith, slated for theater release in December 2015. Hopefully this will raise even more awareness to TBI (traumatic brain injury), and remember, minimal TBI falls into these categories and discussions.
Here is just a small sampling of some of the complications of concussions on human gait. Head injuries are no joke, their effects on dynamic motor control and sensory-motor integration are potentially serious issues. From the first 4 references that came up on the pubmed search this is what was mentioned:
- “the ability to control and maintain stability in the frontal plane during walking is diminished under divided attention” (1)
- “Adolescents with concussion displayed increased center-of-mass medial/lateral displacement and velocity during dual-task walking after RTA (return to activity), suggesting a regression of recovery in gait balance control. This study reinforces the need for a multifaceted approach to concussion management and continued monitoring beyond the point of clinical recovery.” (2)
- “concussion may have long-term observable and measurable effects on the control of gait stability”(3)
- “persons with a history of concussion adopt a more conservative gait strategy”.(4)
Do you see something strange on your client’s gait analysis ? Have you asked them about previous concussions and head injuries? Perhaps you should. Take mTBI seriously, this is not a trivial matter.
Dr. Shawn Allen, one of the gait guys
References:
1. Clin Biomech (Bristol, Avon). 2005 May;20(4):389-95. Epub 2005 Jan 28.The effect of divided attention on gait stability following concussion.Parker TM1, Osternig LR, Lee HJ, Donkelaar Pv, Chou LS.
2. Med Sci Sports Exerc. 2015 Apr;47(4):673-80. doi: 10.1249/MSS.0000000000000462.Return to activity after concussion affects dual-task gait balance control recovery.Howell DR1, Osternig LR, Chou LS.
3.Med Sci Sports Exerc. 2006 Jun;38(6):1032-40.Gait stability following concussion.Parker TM1, Osternig LR, VAN Donkelaar P, Chou LS.
4. Arch Phys Med Rehabil. 2011 Apr;92(4):585-9. doi: 10.1016/j.apmr.2010.11.029.The chronic effects of concussion on gait.Martini DN1, Sabin MJ, DePesa SA, Leal EW, Negrete TN, Sosnoff JJ, Broglio SP.
Just when do those hamstrings fire anyway? In a follow up to mondays post, check out what the EMG studies say..


Pincher nails. Who knew !?
Written by Dr. Shawn Allen
*note: there are two photos here in today’s blog post, look for the side scroll arrows and click on the small box in the upper left corner if you cannot see the photo
We have seen this one for years in our clinics but we never got around to researching it and pondering the condition more deeply. Here is our mantra for today, Form follows Function.
Studies seem to be undecided on the cause of this entity. Some suggest that pincer nails are caused by lack of upward mechanical forces on the toe pad where others remark that they can be observed amongst the healthy mechanical walkers. Hitomi’s study suggests that the affected toes fail to receive adequate physical stimulation from proper toe and forefoot loading. Please read on, this gets interesting.
According to Hitomi’s study, in both the barefoot and shod state,
“the pincer nail group had significantly lower pressure on the first toe than the control group. In both the barefoot and shod state, the peak pressure area was mostly the metatarsal head area in the pincer nail group, whereas it was mostly the first toe area in the control group. Binomial logistic regression analysis revealed that peak pressure area was a significant risk factor for pincer nail development.”
This seems to suggest that there is insufficient or aberrant use of downward pressure on the toes and into the toe pads. Hitomi speaks of the locale of the peak pressure, seemingly proposing from this study that it should not be under the metatarsal heads. This, in our experience and thinking, could suggest that more long flexor dominance is present. This long flexor activity seems to create some disfunction not only in the activity of the lumbrical muscles but also altered pressures in the metatarsal (MET) heads. It certainly alters distal toe pressures which can alter skin and nail responses (see our blog post on subungal hematomas for more on this topic where we discuss principles of counter pressure and shear forces). We try to teach a “spread and reach with long flat toes” approach to our clients in correcting bad habits such as toe hammering and gripping (which are often a result of flawed biomechanics elsewhere).
The nail bed is very rich in vasculature (hence the cause of the dreaded hematoma, the black toenail) and nerve endings. The nail bed is a derivative of the epidermis containing keratin which gives it its hard nature. The nail consists of the nail plate, the nail fold, the nail matrix, the sterile matrix and the hyponychium. There are many factors that go into the formation of a normal nail, including blood flow, nutrition, local neurogenic factors and not to forget, mechanical loading issues. Failure of any of these issues can lead to softening, brittle, thinning, diseased or malformed nails. The nail grows from a nail root in front of the cuticle and grows distally at a slow but (usually) steady rate. It is interesting to note that the long extensor tendon (EDL) attachment is close to the proximal nail bed root area thus it brings forward thinking of possible imbalances between long and short flexors and extensor tendons/muscles and their patterns of imbalance in toe gripping and hammering that could cause a change in function which could drive a change in form. We have all heard it, form follows function, why should this area be any different ?
Hitomi also mentioned something interesting in his study, the observation that bed ridden clients seem to have a predilection to pincer toes. This at least seems to fit the aberrant loading patterns, in this case an absence of. The study also started some interesting thinking in us when it mentioned a hypothesis,
“that human nails are constitutively equipped with an automatic shrinkage function that allows them to adapt to daily upward mechanical forces.”
This was a fascinating hypothesis to us. It seems to make sense. If constant downward pressure on the toe pads were present, the toe nails would always be undergoing a flattening and spreading response so it could make sense that the nails have a built in curve and shrinkage function offsetting and adapting to the constant distorting pressures (the flattening and spreading forces). Hence, some possible clarity in Hitomi’s hypothesis that pincer nails are caused by lack of (and in our thinking, distorted) upward mechanical forces on the toe pad. And, when those distorting pressures are placed elsewhere (ie. the MET heads or tips of the toes as in our subungal hematoma hypothesis) or faulting gripping or hammering loading the automatic shrinkage function is left to dominate.
We think Hitomi’s hypothesis is correct. Here is why (this is paraphrased from our blog post on subungal hematomas and our revolutionary thinking on why they occur and it seems to fit well with pincer nail formation as well).
… when the skin is pulled at a differential rate over the distal phalange (from gripping of the toes rather than downward pressing through the toe pad) there will be a net lifting response of the nail from its bed as the skin is drawn forward of the backward drawn phalange (there is a NET movement of skin forward thus lifting the nail from its bedding). For an at-home example of this, put your hand AND fingers flat on a table top. Now activate JUST your distal long finger flexors so that only the tip of the fingers are in contact with the table top (there will be a small lifting of the fingers). There should be minimal flexion of the distal fingers at this point. Note the spreading and flattening of the nail. Now, without letting the finger tip-skin contact point move at all from the table, go ahead and increase your long flexor tone/pull fairly aggressively. You are in essence trying to pull the finger backward into flexion while leaving the skin pad in the same place on the table. Feel the pressure building under the distal tip of the finger nail as the skin is RELATIVELY drawn forward.] This is fat pad and skin being drawn forward (relative to the phalange bone being drawn backward) into the apex of the nail. Could this be magnifying the curvature of the nail and not offsetting the “automatic curving and shrinkage” function of the nail ? We think it is quite possible.
So, there you have it. We will dive deeper on this topic another time, but after reading Hitomi’s study our brain’s started buzzing because we had discussed this process similarly a few years back in our Subungal Hematoma blog post.
And, if you are thinking about chronic repeated ingrown toe nails with this clinical entity, your thoughts are clearly on a logical path. There is a correlation it seems.
And, as for the horrific metal bar correction you see in the other photo above, this too is new to our eyes. It seems rather medieval, something one might see in the gallows of yesteryear. And if that doesn’t curl your hair and make you nauseated, try looking at what this one guy did, a DIY remedy (caution, not for the feint of heart). https://www.mja.com.au/journal/2005/182/4/diy-pincer-nail-repair-brace-yourself
ShawnAllen, one of the gait guys
References:
Foot loading is different in people with and without pincer nails: a case control study Hitomi Sano1*, Kaori Shionoya2 and Rei Ogawa1 Journal of Foot and Ankle Research 2015, 8:43
Hamstring Reverse Engineering:
The biceps femoris is an internal rotator of the thigh? You heard correctly. Think of how the lower extremity works in closed chain, not open. Check out this quick video with Dr Ivo on “reverse engineering”

What creates muscle tone, anyway?
Not for the timid, here is an excellent , free, full text article on spasticity. More importantly, it is an excellent review on what creates muscle tone and how it is maintained, starting and the spindle and moving centrally. Think about this the next time you have a patient with mm spasm and you can se things in a whole new light

Irregular Arm Swing Could Be Early Sign Of Pending neurological disease.
Written by Dr. Shawn Allen
We’ve been saying this for quite some time now, the small subtle gait changes are often the first sign of things to come.
The attached article suggests that scientific measurement investigating irregular arm swing during gait could help diagnose the Parkinson’s disease earlier, giving greater opportunity to slow brain cell damage and disease progression.
In the study below Huang suggests that although we all know that classically the Parkinsonian disease is met with tremors, slow movements, stooped posture, rigid muscles, bradykinesia, speech changes etc, “by the time we diagnose the disease, about 50 to 80 percent of the critical cells called dopamine neurons are already dead,”
Previously, here at The Gait Guys, we have gone deep into discussions of arm swing and the phasic and anti-phasic natures of limb action in gait and how the four limbs interact neurologically, both centrally and peripherally. You can click here for just a sampling of our “arm swing” writings,
In the study, because arm swing changes are one of the first gait parameters to diminish and decline, and because the decline is typically asymmetrical due to the fact that the disease is an asymmetrical one, the authors compared arm swing magnitude and asymmetry in patients with and without Parkinson’s as parameters to begin the assessments. Most research to date has commented on the early loss of arm pendular swing but as they said here, “ but nobody had looked using a scientifically measured approach to see if the loss was asymmetrical or when this asymmetry first showed up,“ explained Huang.
What they discovered was that compared to the control group, “the Parkinson’s group showed significantly greater asymmetry in their arm swing (one arm swung significantly less than the other while walking),” and when the subjects walked faster, the arm swing increased but the amount of asymmetry remained unchanged.
On a slightly different tangent of thinking, an aside from the Parkinson’s disease disucussion, how truly sensitive is this limb swing thing you might ask ? Here, read this from this piece (How injury and pain reorganize the brain) we wrote a few years ago.
“Getting a cast or splint causes the brain to rapidly shift its resources to make righties function better as lefties, researchers found.
Right-handed individuals whose dominant arm had to be immobilized after an injury showed a drop in (brain) cortical thickness in the area that controls primary motor and sensory areas for the hand, Nicolas Langer, MSc, of the University of Zurich in Switzerland, and colleagues reported.
Over the same two-week period, white and gray matter increased in the areas that controlled the uninjured left hand, suggesting “skill transfer from the right to the left hand,” the group reported in the Jan. 17 issue of Neurology.
The findings highlight the plasticity of the brain in rapidly adapting to changing demands, but also hold implications for clinical practice, they noted.”This article highlights the rapid changes in motor programs that occur. It does not take long for the body to begin to develop not only functional adaptations but neurologic changes at the brain level within days and certainly less than 2 weeks.
If you know your literature on this topic of arm swing symmetry, you know it is an arguable point. According to the Lathrop-Lambach study (see link in the article just mentioned above), they mentioned that they feel a 10% baseline asymmetry is the norm. This symmetry issue is an arguable point that no one is likely to ever win. We tend to feel, as many others do, that asymmetry can be a major component and predictor to injury, and in today’s topic of discussion a possible determinant of higher level gait disease.
Still think you should retrain arm swing ? Dive into our blog archives here on arm swing, you will find out that perhaps it is not your best first choice. Discover from our old writings who tends to dictate how much arm swing occurs.
Shawn Allen, one of the gait guys
References:
http://www.medicalnewstoday.com/articles/173680.php
“Arm swing magnitude and asymmetry during gait in the early stages of Parkinson’s disease.”
Michael D Lewek, Roxanne Poole, Julia Johnson, Omar Halawa, Xuemei Huang
Gait & Posture, 2009, In Press, Corrected Proof, Available online 27 November 2009 DOI:10.1016/j.gaitpost.2009.10.013

Does gait (re)training alter peoples biomechanics?
You bet it does! Should we be retraining peoples gait? We like to think, yes. What do you think?
“Overall, this systematic review shows that many biomechanical parameters can be altered by running modification training programmes. These interventions result in short term small to large effects on kinetic, kinematic and spatiotemporal outcomes during running. In general, runners tend to employ a distal strategy of gait modification unless given specific cues. The most effective strategy for reducing high-risk factors for running-related injury-such as impact loading-was through real-time feedback of kinetics and/or kinematics.’
Br J Sports Med. 2015 Jun 23. pii: bjsports-2014-094393. doi: 10.1136/bjsports-2014-094393. [Epub ahead of print]
Gait modifications to change lower extremity gait biomechanics in runners: a systematic review.
Napier C1, Cochrane CK1, Taunton JE2, Hunt MA1.
A nice, referenced piece from one of our fav’s, Dr Michaud.
“Although early research suggested a limited connection between arch height and lower extremity function, more recent research confirms that arch height does indeed affect function. Information obtained from measurements that accurately identify the height of the medial longitudinal arch may lead to more effective treatment protocols. By identifying specific injuries associated with low and high arches, it may also be possible to prevent these injuries.”
Reciprocal Inhibition anyone? Thanks to The Manual Therapist (Erson Religioso) for this great post.
What they are doing here is taking advantage of what Sherrington know many years ago. Activating a muscle (agonist for a movement) will inhibit the muscle with the opposite action (antagonist for a movement), through a disynaptic, post synaptic pathway. It is a great way to gain additional movement and remove or reduce muscular inhibition. Try it!

Donate here











Help keep us free ! Make a donation by clicking. here.

Donate to get exclusive content from The Gait Guys
OUR SEARCH BOX IS INTUITIVE, TYPE IN YOUR KEY WORD, WAIT, THEN SCROLL DOWN.
Email us: our email is found under the "Disclaimer" Tab above.

Powered by Squarespace.