

Using a Pedograph to get Dynamic Answers to Foot Dysfunction:
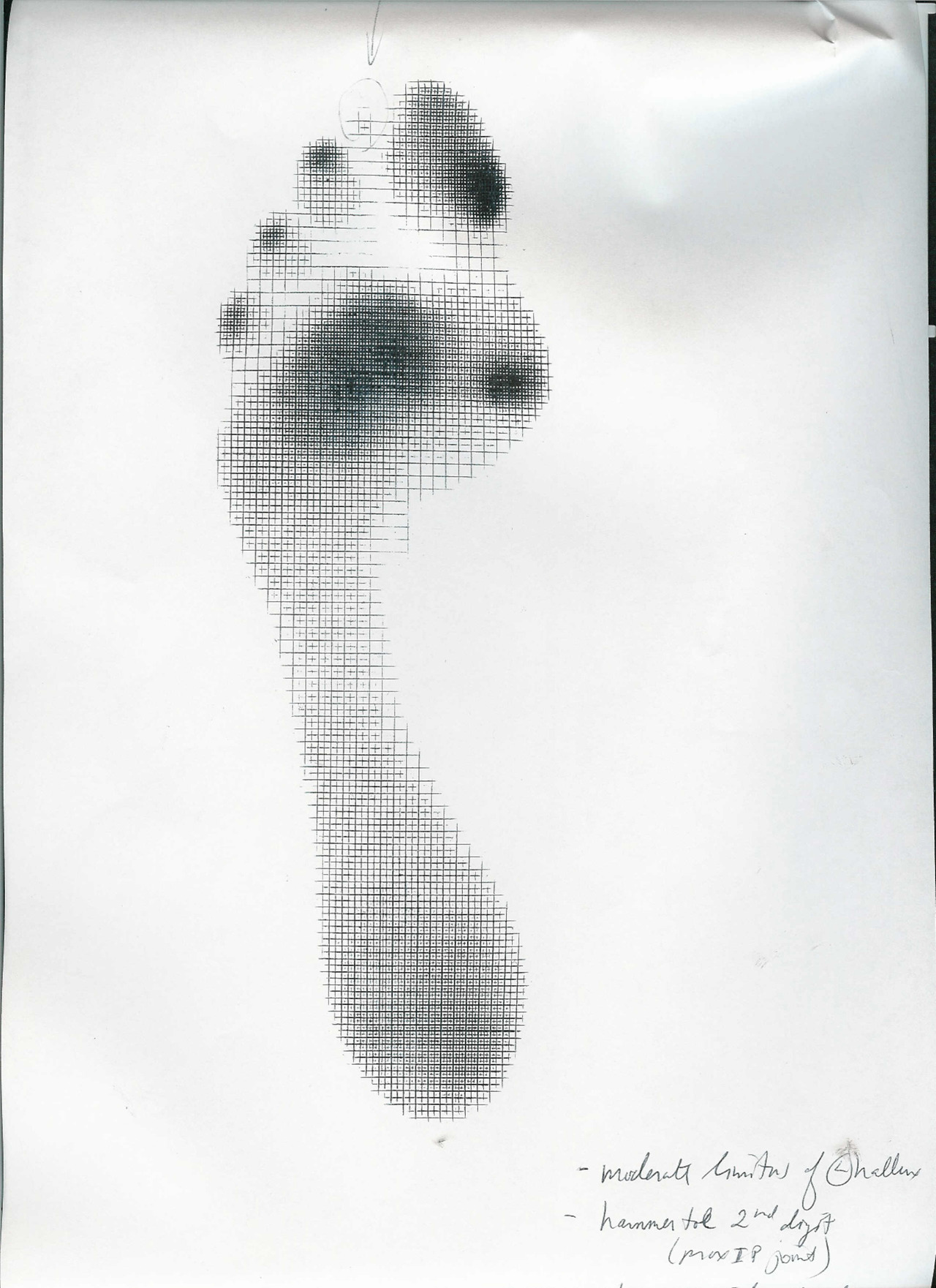
Pedograph topic: One quick topic here. Note the hot spot (ink concentration) at the big toe and note that the ink is proximal on the toe pad. We would like to see the pressure point at the center of the pad. This spot means this person walked across the Harris Ink mat with increased FHB (flexor hallucis brevis) use and not enough FHL (flexor hallucis longus); too much short flexor, not enough long flexor. There is loss of synergy between the two. This will likely mean there is something going on in the extensors as well, something abnormal.
Need a review? Look at Monday’s video again on the EHB (extensor hallucis brevis) where we discuss all of the toes muscles.
Clinically this patient had a hallux limitus/rigidus (could not dorsiflex great toe) which complicated the mechanics at the joint and forward into the great toe, sadly also at the foot’s medial tripod as well. You cannot get an accurate read from a static (standing only) pressure mapping. Don’t rely on them for dynamic info !
Too much FHB with not enough FHL means EHB (as well as long extensors of the lesser toes) is going to be impaired. Impair the EHB and you ask the EHL to work differently as well. Here’s a hint, look at all the printing under the lesser digits distally, there is too much flexor activity here as indicated by intense inking from toe clenching / hammering. They are likely doing this to add more stability since the great toe cannot from what we discussed above. There are problems that come from these issues as well but we want to stay focused on the big toe today.
Now, go back and review Mondays blog video post (here is the link).
Treatment:
In a case where there is some loss of the 1st MPJ range of motion (metatarsaphalangeal joint) (depending on the source, 45 degrees is typically needed) there will be impairment of the long and short toe flexor/extensor pairing and synergy. In this case above there is highly suspected increased short flexor (FHB) activity (hence the ink at the proximal big toe) and this means that the long flexor is usually submissive. And, when the long flexor (FHL) is submissive the long extensor is dominant. When the long extensor is dominant the short extensor is submissive. Can you now see the beautiful symphony and harmony we need here. This is why we loosely say that the FHB and the EHL are paired and the FHL and EHB are paired. It is not exactly the case but hopefully you catch our drift.
So, in this case, with a hallux limitus/rigidus when the 45 degrees of dorsiflexion is lost these pairing can be challenges and the synergy is lost. The symphony of these muscles is “off tune”. This can further provoke the 1st MPJ and it can also be the slow brewing initiation of the problem. It can be a vicious cycle when it gets going. And, when the 1st MPJ is limited the dorsiflexion that is supposed to occur at the joint can be shunted proximally into the midfoot or ankle and cause pain/pathology there. It can also impair the normal pronation-supination cycles. The big toe when it goes sour makes the whole orchestra angry and play off tune.
Doing your best to normalize and maximize muscle harmony and function many times will dampen the pathology and pain and get the person going again. Of course the problem is still lurking under the surface. Test the muscles, try to isolate them but remember that your muscle tests need to be as specific as you can. Nothing is isolated in the body, but do your best.
Of course there are many other scenarios but this is the one we chose to teach today from this pedographing of the big toe. We will explore other options and challenges another time.
Shawn and Ivo. Gait geeks promoting gait literacy and competency everywhere we can get an open ear.













