

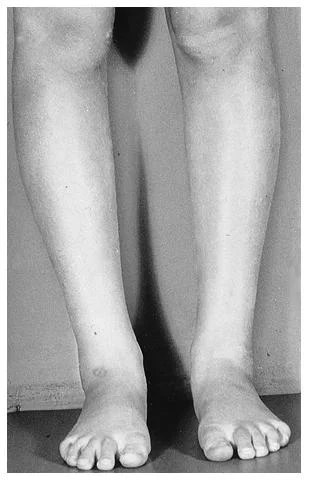

Photographs of a 6 yr. old.
What do you see ? How does the alignment look ? Are they developing normally ?
At what point should you intervene to ensure proper alignment and
development occurs in this child ? Can we standardize our visual
screen to fit all cases in all children ? So many questions !
* this case goes very nicely with a prior case on the blog published on July 15th.
Click back and forth between the two photos above on the blog. Youcan see that in the first photo that when the feet are parallel, the patellae point inward (normal compensation).
In photo 2, we can see that when we put the patellae in the saggittal plane (pointing
forward) the foot progression angle is severely positive (externally postured or out-toed).
This is a severe case of FEMORAL ANTETORSION
with compensatory EXTERNAL TIBIAL TORSION. The external tibial
torsion is an external spin along the long axis of the shaft in a
response to try to correct alignment. You can see that in this case
there is no happy medium. The torsion in the long bones is so extreme
that either the knees are positioned inwards when the feet are
normally aligned or the feet are spun outwards when the knees are
properly aligned. Regardless, there is much abnormal stress on the
hip and knee joints and the labrum of the hip and menisci of the knees
not to mention the challenges into the foot mechanics and gait.
______________________________
Taking this into a gait perspective:
Patients with antetorsion are forced to externally rotate the limbs to bring the knee forward to a normal alignment from an internally rotated position.
This takes up some, occasionally all, of the lateral (external) rotation needed for the hips to function normally during gait causing compensatory rotation of the spine during single leg stance; the spine being really the only place the rotation can be achieved.
Normally, during gait the hip rotates laterally from toe off through to heel strike and is present during the initial loading response.
When this rotation does not occur in the hip, it must occur as a compensatory motion somewhere else in the kinetic chain and this is usually the pelvis or lumbar spinal joints.
Furthermore, the abnormal alignment of the femoral head in the acetabulum can repetitively irritate the hip joint and labrum let alone place abnormal torque on the tib-femoral joint (knee).
Antetorsion patients who compensate and realign the feet to a normal progression angle via tibial external torsion will force the femoral head anteriorly into the anterior hip capsule and this is a common source of pain. It is a “hammocking effect” into the anterior capsule and it can leave the femoral head and it’s cartilage uncovered and uncompressed thus advancing arthritis degeneration.
This is a similar symptom phenomenon as in “anterior femoral glide syndrome” as described by Shirley Sahrmann. It is not uncommon to see a sway back lumbar posture in these clients.
These patients may have anterior contractile tissue deficits, namely stretch-weak iliopsoas as described by Kendall.
Remember to check for limb length symmetry in these clients who’s anteversion is not symmetrical.
Watch for a future series on torsions and versions
We may be twisted, but the last time we looked, we are still …… The Gait Guys













