The power to bend bones.
What have we here? Hmmm. This little girl was brought in by her mother because of intermittent knee pain and “collapsing” of the knees while walking, for no apparent reason.
The ankle dorsi flexion (or ankle rocker; see last 2 pictures; we are fully dorsiflexing the ankles) needs to occur somewhere, how about the knees? Or in this case, the tibia. Wow!
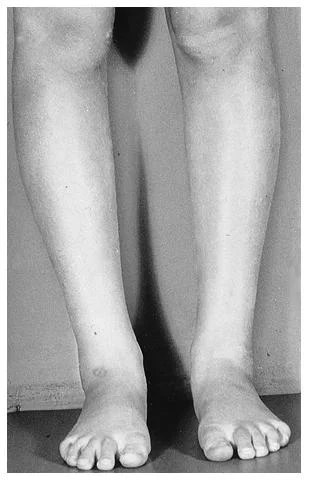
You are looking at a 4 year year with a condition called genu (and tibial) recurvatum. Genu recurvatum is operationally defined as knee hyperextension greater than 5 degrees. The knee is hyperextended, and in this case, the tibia is literally “bent backward”. Look at the 2 pictures of her tibia.
Generally speaking, the tibial plateau usually has a slight posterior inclination (as it does in this case; look carefully at the 1st picture) causing the knee to flex slightly when standing. Sometimes, if it is parallel with the ground and the center of gravity is forward of the knees, the knee will hyperextend (or in this case, the tibia will bend) to compensate.
In this particular case, the tibia has compensated more, rather than the knee itself. The knee joint is stable and there is no ligamentous laxity as of yet. She does not have a neurological disorder, neuromuscular disease or connective tissue disorder. She has congenitally tight calves.
As you can imagine, her step length is abbreviated and ankle rocker is impaired.
So what did we tell her Mom?
- keep her barefoot as much as possible (incidentally, she loves to be barefoot most of the time, gee, go figure!)
- have her walk on her heels (she’s a kid, make a game of it)
- showed her how to do calf stretches
- balance on 1 leg with her eyes open and closed
- keep her out of backless shoes (like the clogs she came in with)
- keep her out of flip flops and sandals where she would have to “scrunch” her toes to keep them on.
- follow back in 3 months to reassess
There you have it. Next time you don’t think Wolff’s (or Davis’s) law* is real, think about this case. Want to know more? Consider taking our National Shoe Fit Program, available by clicking here.
The Gait Guys. Making you gait IQ higher with each post.
*Wolff’s law: Bone will be deposited in areas of stress and removed in areas of strain. or put another way: bone in a healthy person or animal will adapt to the loads under which it is placed
Davis’s law: soft tissue will adapt to the loads that are placed on it