Gait: When loading COM (center of mass) gets complicated.
/When loading COM (center of mass) gets complicated.

Wednesday night on our monthly seminar we discussed some problems with different foot types and how they might load differently compared to others, possible sources of pathology and why someone might have challenges or different strategies in loading the limb over a given foot type. This is just another reason why blanket statements like load the "head over foot" just cannot be made. The COM (center of mass) is subservient to many variables, including how the foot loads, and where its foot loading target is in the step width realm. One just cannot tell or teach everyone to load the head over the foot, it is just foolish to put everyone in that blanket category (besides, it is a category we do not believe is proper or safe). There are just too many variables (genu varum, genu valgum, tibial torsion, femoral torsion, foot types such as rear or forefoot varus or valgus or forefoot supinatus, etc.). The only article we have ever read even suggesting "head over foot", actually said, COM "outside the foot", and that was only during running initiation, the first steps, to get propulsion going, it is not the way we are to run. And over the next few weeks we will continue to write about the problems and repercussions of a COM drift over the foot.
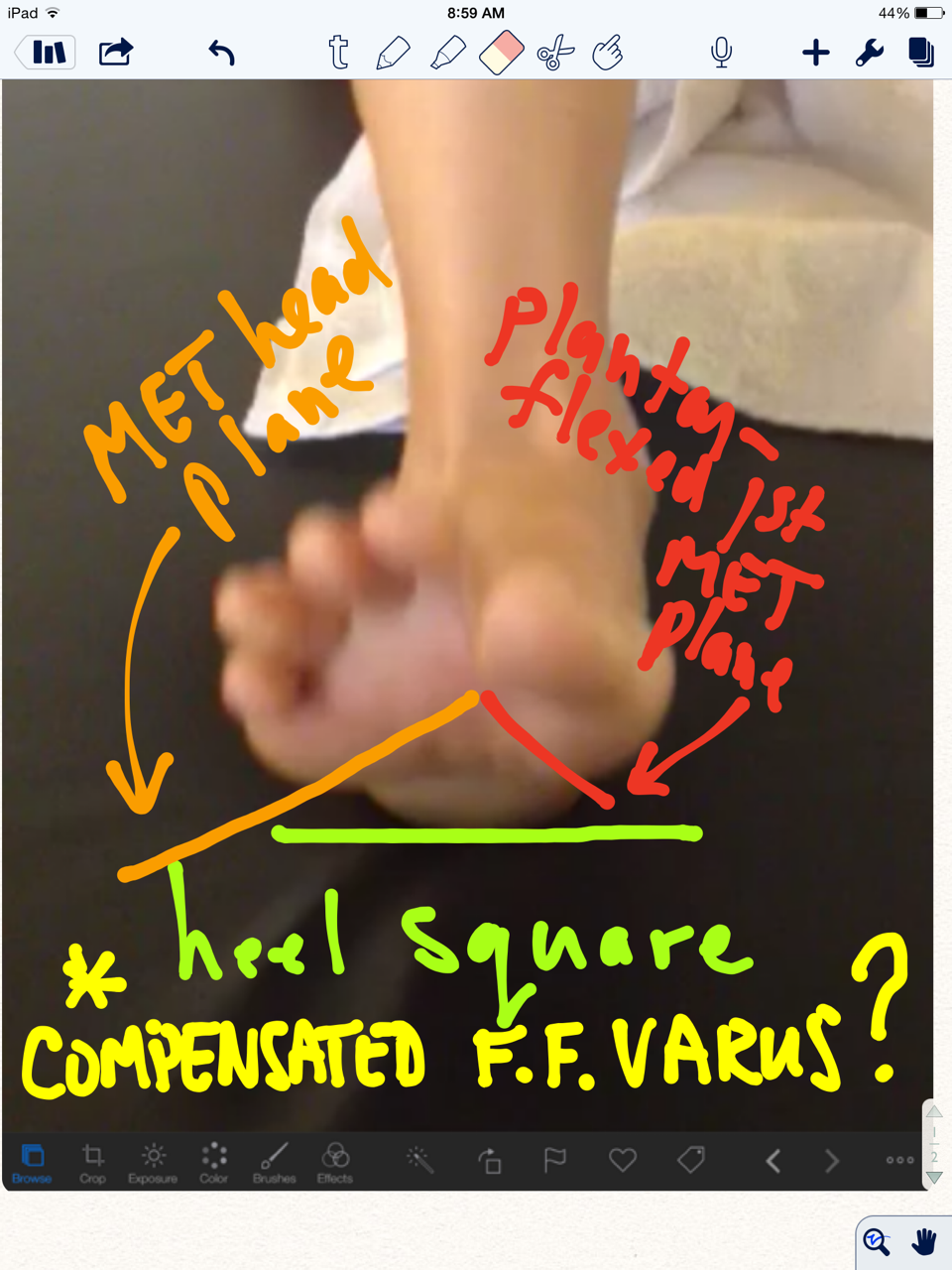
Here was a slide from last night, this is supposedly a drawing of a neutral rearfoot-forefoot relationship, and a relatively neutral pedo mapping of a supposedly neutral foot. But think about this, just because unloaded, during your examination, the foot appears neutral does it mean it will load in that neutral manner. It appears neutral in passive ROM assessment, but under dynamic loading the game can be completely different. For example, what if the tibialis posterior is insufficient? In those cases the rear foot may not support inversion, it might actually valgus load, this can force the loading into premature and sustained pronation issues. Now mind you, if the pedo mapping is dynamic, like we teach it, you will get much of the movement (and compensation) info on the mapping, but many teach static mapping (stand on this, just stand, no walking across it).
But this all comes back to what we say in gait analysis, "what you see is often not the problem, it is the compensation". This is why one must compare one's exam to the dynamic loading challenges your assessment should include, including gait observation. This is also why one is foolish to make gait recommendation off of just what one sees in someone's gait, because you can be recommending changes to an already compensated gait. Just because you think someone will load better in a manner in which you think is better does it mean they can, are able, or capable of doing so without compensation or tissue compromise.
Caveat emptor, and more so, Caveat Venditor (buyer beware, and more so, seller beware).