Ankle inversion sprain ? or off-loading photo ?
/How we do one thing, is how we do all things.

I was sitting having my morning coffee earlier than normal this morning, which left me time to ponder some things.
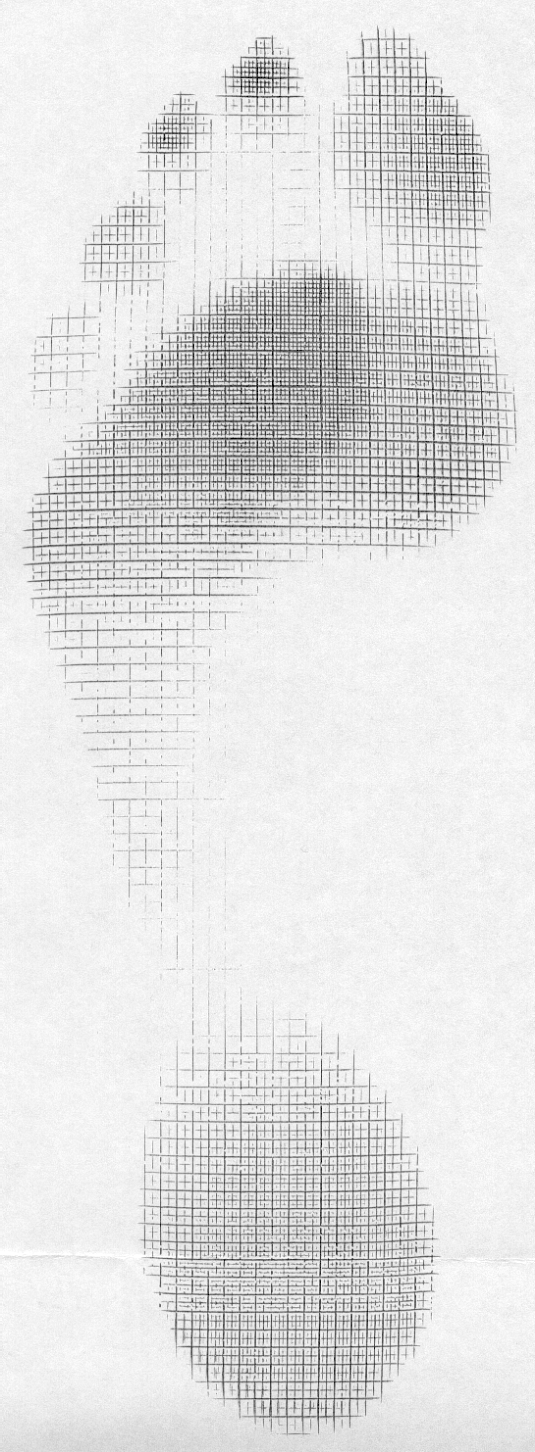
Look at this picture, is this not a magnification of the "cross over gait" x100 ? Thus, is that planted foot not inverted ? Yes, it has to be, to a degree, a high degree. There is a reason why soccer players have a great affinity for ankle sprains.
When we have a narrow based gait, we are most likely going to strike more laterally on the foot, more supinated, if you will. If you widen step width, less inversion, less lateral forces (typically) and less supination (typically) compared to a narrow based gait.
If we descend stairs with our feet in a more narrow based gait, we are not only going to be inverted more, but striking at the ball of the foot, thus, more on the lateral foot tripod. This is the typical inversion sprain injury position.
When we jump, we should be trying to land with our feet more abducted, certainly not narrow based, because if we are too narrow we are at more risk for the same lateral forefoot landing and thus ankle inversion event. Just like descending stairs.
We see plenty of ankle inversion events. Why?
Because most people do not have enough hip abduction or peroneal skill, strength, endurance and they are unaware of their weak gait patterns or their ankle spatial awareness. Many have lazy narrow based gaits and insufficient proprioceptive awareness. And, they carry these things over into running, walking, jump landing (ie. volleyball, basketball, etc), and descending stairs, just to name a few.
How we do one thing, is how we do all things (mostly).
Rickie Lovell As he struck the ball it would been everted. The momentum of the follow through will have off loaded the everted foot as the energy moves in a similar line to that of the ball. It is extremely rare for a footballer to get a sprain from this, I certainly didn't see over several years working in professional football.
On a side note, find some footage of David Beckham taking free kicks - the mechanics are astounding!
The Gait Guys possibly everted, but no guarantee.It still looks pretty inverted to me.But we see your point, and is a real good one, real good. Super good. We will check our the bender-man thanks for chiming in with such great insight !
The Gait Guys yes, the momentum of the leg kicking across the body would externally spin the stance leg. The picture is likely showing the offloading phase, not the loadin
Rickie Lovell The benefits of being a Brit that used to play!