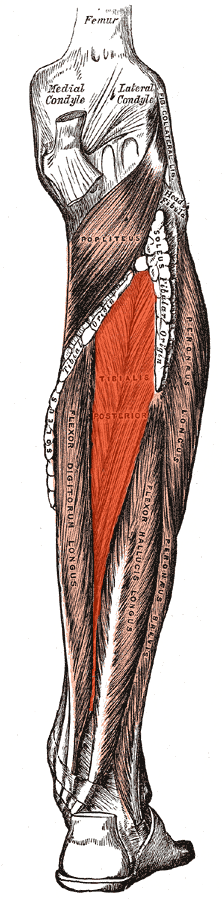
A little more on the tibialis posterior (or any tendon for that matter)....
/
We tend to think of the etiology of tendinopathies as being overuse or biomecanically stressful situations, which are often true, but have you thought about vascularization? My partner Dr Allen wrote a great post on vascularization in a yo yo professional here. It has to make you think...
I wrote about posterior tibial tendinopathies in a post a few days ago. A recent paper shows that vascularization can be a major player in posterior tibial tendinopathies (1). Tendon blood flow tends to decrease with age and compression, which often results from increased mechanical load. This decreased vascularization, at least theoretically, can contribuute to the probability of tissue damage as tissue compliance and flexibilty will be compromised (LER). Oxygen consumption of ligaments and tendons is 7.5% lower than skeletal muscle, which may contribute to longer healing times (2,3).
So, how can we increase vascularization?
- Aerobic conditioning increases mitochondrial content, myoglobin content and capillary number, among other things, due to increased demand (4).
- Manipulation, mobilization and massage, locally as well as segmentally, can increase blood flow, at least temporarily (5,6). The L4-S1 segments of the posterior tibial nerve are the segmental levels for the tibialis posterior .
- How about some moist heat to cause local peripheral vasodilation?
- I wrote a commentary on how needling can effect local vasodilation here (7), based on this article (8).
- Tissue engineering with various techniques is an upcoming and promising field (9)
- the early research on laser therapy (photobiomodulation) has shown some positive outcomes (10)
Finally, there is some great information about medications and current research from The Angiogenesis Foundation (11)
Adding a modality like needling or acupuncture, combined with exercise and some moist heat and perhaps some laser may help to improve your outcomes. There appears only upside potential and the methods are easy to apply and implement.
1. Geideman WM, Johnson JE. Posterior tibial tendon dysfunction. J Orthop Sports Phys Ther 2000;30(2):68‐
2. Patla CE, Abbott JH. Tibialis posterior myofascial tightness as a source of heel pain: diagnosis and treatment. J Orthop Sports Phys Ther 2000;30(10):624‐
3. Vailas AC, Tipton CM, Laughlin HL, et al. Physical activity and hypophysectomy on the aerobic capacity of ligaments and tendons. J Appl Physiol 1978;44(4):542-546.
4. https://www.cdc.gov/nccdphp/.../chap3.pdf
5.Pickar JG Neurophysiological effects of spinal manipulation. Spine J. 2002 Sep-Oct;2(5):357-71.
6. http://emedicine.medscape.com/article/324694-overview
7. http://www.rehabchalktalk.com/dry-needling-and-vascular-changes
8. BMC Complement Altern Med. 2015; 15: 72. Published online 2015 Mar 20. doi: 10.1186/s12906-015-0587-6PMCID: PMC4426539 Intensive vasodilatation in the sciatic pain area after dry needling