Join Us Wednesday Evening
/We are doing our monthly lecture on chirocredit.com on Wednesday Evening, 8 PM EST (7 central, 6 mountain, 5 west coast). Get credit and get entertained at the same time. Look for Biomechanics 311
Aloha
Ivo and Shawn
We are doing our monthly lecture on chirocredit.com on Wednesday Evening, 8 PM EST (7 central, 6 mountain, 5 west coast). Get credit and get entertained at the same time. Look for Biomechanics 311
Aloha
Ivo and Shawn

The Power of Facilitation: How to supercharge your run.
While running intervals this crisp, cool 19 degree morning, something dawned on me. My left knee was hurting from some patellar tracking issues, but only on initial contact and toe off. I generally run with a midfoot strike. I began concentrating on my feet, lifted and spread my toes and voila! my knee pain instantly improved. Very cool, and that is why I am writing this today.
Without getting bogged down in the mire of quad/hamstring facilitation patterns, lets look at what happened.
I contracted the long extensors of the toes: the extensor digitorum longus and the extensor hallicus longus; the short extensors of my toes: the extensor digitorum brevis, the extensor hallucis brevis: as well as the dorsal interossei.the peroneus longus, brevis and tertius were probably involved as well.
Do you note a central theme here? They are all extensors. So what, you say. Hmmm…
Lets think about this from a neurological perspective:
In the nervous system, we have 2 principles called convergence and divergence. Convergence is when many neurons synapse on one (or a group of fewer) neuron(s). It takes information and “simplifies” it, making information processing easier or more streamlined. Divergence is the opposite, where one(or a few) neurons synapse on a larger group. It takes information and makes it more complicated, or offers it more options.
In the spinal cord, motor neurons are arranged in sections or “pools” as we like to call them in the gray matter of the cord. These pools receive afferent information and perform segmental processing (all the info coming in at that spinal cord segment) before the information travels up to higher centers (like the cerebellum and cortex). One of these pools fires the extensor muscles and another fires the flexor muscles..
If someone in the movie theater keeps kicking the back of our seat, after a while, you will say (or do) something to try and get them to stop. You have reached the threshold of your patience. Neurons also have a threshold for firing. If they don’t reach threshold, they don’t fire; to them it is black and white. Stimuli applied to the neuron either takes them closer to or farther from threshold. When a stimulus takes them closer to firing, we say they are “facilitating” the neuron. If it affects a “pool” of neurons, then that neuronal pool is facilitated. If that pool of neurons happens to fire extensor muscles, then that “extensor pool” is facilitated.
When I consciously fired my extensor muscles, two things happened: 1. Through divergence, I sent information from my brain (fewer neurons in the cortico spinal pathway) to the motor neuron pools of my extensor muscles (larger groups of motor neurons) facilitating them and bringing them closer to threshold for firing and 2. When my extensor muscles fired, they sent that information (via muscle spindles, golgi tendon organs, joint mechnoreceptors, etc) back to my cerebellum, brain stem and cortex (convergence) to monitor and modulate the response.
When I fired my extensor muscles, I facilitated ALL the neuronal pools of ALL the extensors of the foot and lower kinetic chain. This was enough to create balance between my flexors and extensors and normalize my knee mechanics.
If you have followed us for any amount of time, you know that it is often “all about the extensors” and this post exemplifies that fact.
Next time you are running, have a consciousness of your extensors. Think about lifting and spreading our toes, or consciously not clenching them. Attempt to dorsiflex your ankles and engage your glutes. It just may make your knees feel better!
The Gait Guys. Facilitating your neuronal pools with each and every post.
All material copyright 2013 The Gait Guys/ The Homunculus Group. All rights reserved. If you rip off our stuff, we will send Lee after you!
Today we talk about many things affecting, impairing, and relating to ankle dorsiflexion, and so much more ! Join us today on The Gait Guys podcast !
A. Link to our server:
http://thegaitguys.libsyn.com/podcast-41-the-ankle-dorsiflexion-podcast
B. iTunes link:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138
C. Gait Guys online /download store (National Shoe Fit Certification and more !) :
http://store.payloadz.com/results/results.aspx?m=80204
D. other web based Gait Guys lectures:
www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
________________________________________
* Today’s show notes:
Neuroscience:
Hello there, I’ve been following your stuff for a while now after searching far and wide for solutions to issues I have with my feet/ankles (and the fact I have an interest in what you guys do, I’m going to University in two weeks to study Sports Therapy).
Why I decided to message you now though is because …
8. Disclaimer
9. National Shoe Fit program and our Payloadz store
10. Online CE October 30th
11. In the media:
Achilles pain and glute control

Look at these kids running … all but one shows poor form, but remember, these kids are still undergoing neurodevelopment and are learning to control their body parts. Remember, the maturation/myelination of the nervous system usually lags behind the development of the musculoskeletal system.
In the photo, lets first focus on the happy lad in the green shirt. He sure looks like he is having fun, which is what running should be about in kids. If you try to make running a chore for kids you just might lose their love of it in the process. But our point here at The Gait Guys is to teach. So here in this photo are some good teaching points. You should see:
1- the stance phase leg (right leg) is spun out into external rotation. Not too much of a big deal because we do not know if he has finished the normal derotation process of the limb, sometimes this can carry into the puberty years even though for most kids the process is largely completed by his predicted age.
2- The pelvis has drifted laterally in the frontal plane past a perpendicular line up from his foot. This could mean alot of things including gluteus medius or abdominal weakness but the point here is that he has broken through the lateral line (frontal plane) of support up through the hip-pelvis-core chain. This is going to set up what the the left knee (swing leg) is doing and will set up #3.
3. Cross over gait is virtually guaranteed because of the lateral pelvis drift as noted in #2. It is virtually guaranteed as well because the swlng leg knee coming inwards is dictating it. IF the knee is coming inwards toward the midline the thing attached to it , the foot, is going to follow. The swing leg is a pendulum, if you shift the pivot point of the pendulum (in this case to his right) the pendulum will swing to the right. This is a self-perpetuating cycle and it will not correct without strengthening, awareness and drilling positive feedback changes.
4. Dr. Allen’s current thought experiment on Ballasts (see podcast 38) is playing out here with the left arm of this fella. If the pelvis drifts far to the right, the arm will move away from the body to move some of the left side body weight outwards to negate the right shift. This is pure balance physics. Arm swing most of the time cannot be corrected without correcting the thing that causes the aberrant arm swing, and that is often (but not exclusively) aberrant lower limb and pelvis-hip-core or foot mechanics. There are exceptions, but often if you fix the lower limb and pelvis-hip mechanics you will see an immediate change in the arm swing. If you force changes in arm swing without fixing the problem (and that is not to say there are not local arm swing etiologies) you may be driving strength into a compensation pattern that you may not want or like.
5. The girl in the pink tights … . she might have been modelling the boy in the green shirt. Same issues, same concerns.
6. The form we love the most ? The boy in the dark blue shirt and black shorts on the far right. Great form, no major issues here. We bet he didn’t hear the starters gun go off.
On a side note, the fella in the green shirt with that form he would be a champion race walker. He already has the hip action right, the cross over that is loved in that sport and the arm swing. Maybe some exposure to an alternate sport is a better solution here ? Although we are always an advocate for correcting flawed biomechanics.
It is often painful for us to watch kids run. We know that much of the things we hate are temporary because of the neuro-developmental process. But sometimes, if kids run too much at a young age, and are pressed into long running miles or cross country at too young an age, these aberrant mechanics can become their new norm. This is the danger of plasticity in the nervous system. Repeated stimulation of a pattern engrains that pattern and the extent of a brain’s plasticity is dependent on the stage of neuro-development and the brain region affected. When an aberrant running form is allowed to perpetuate into the mid-teenage years, when the majority of the synapses are already formed and neurologic “pruning” and myelination are ramping up, then the repeated exposure to the aberrant pattern can get the myelination. This is the most frustrating thing for us. We would rather see some intervention early on with the creation, strengthening and myelinating of correct motor patterns through skill development training rather than mileage training, rather than discarding the more appropriate synapses that could have, might have, should have, been formed. Our bodies and brain will develop depending on the exposures and demands put upon it. And here is the big key, if you do not clean up someone’s gait aberrancy(s) early on, one should not wonder down the road why they developed flat feet, bunions, early degenerative knees and the like. This is a fairly predictable machine, but you have to try to intervene early to prevent the slings and arrows of outrageous misfortune later on.
Both the brain and the body will adapt to their environment, whether that is an optimal one or a compensatory one. It can myelinate either pathway. Which one will you choose for your kids ?
Shawn and Ivo, The Gait Guys

Do you kick or scrape the inside of your ankle with the other foot ?
We are moving into the final throws of cross country season now and we are seeing the pathologies creep in and the miles go up. Some of you who have been with us for 3 years have seen this picture but we realized we did not have a blog post on the problem represented by this photo. This young runner had these scuff marks on the inside of the right lower leg and ankle after a cross country meet. So what is going on here and what does it tell you ?
Some runners notice that they repeatedly will scuff in the inside ankle or inner calf with the opposite shoe when running. This can happen on both sides but it is more often present unilaterally than bilaterally.
This problem, typically, but not always represents one of two things:
1- cross over gait (if you are new to our blog in the SEARCH box type in “cross over” and “cross over gait” and be sure to see our 3 part video on the cross over on our youtube channel found here).
2- negative foot progression angle which may or may not be combined with a degree of internal tibial torsion. Said easier, the runner is “in-toed” or “pigeon toed” but if you have been here with us awhile on The Gait Guys we expect a diagnosis of a higher order so use the former terms, please.
Lets discuss both.
1- Cross over. When the runner is standing on the right leg, right stance phase of gait, the frontal plane is not properly engaged and the pelvis can drift further over the right foot. This drift to the right will drop the pelvis on the left side. This will alter the pendulum movement of the left leg. Since the global pelvis is moving to the right the left swing leg pendulum moves to the right as well and as it swings past the stance leg it strikes a glancing blow to the inside of the right ankle or calf. This is simple biomechanics and physics. To fix this problem, which is clearly inefficient, one has to determine what is causing the right pelvis drift (there are many causes, the most often thought of cause is a weak gluteus medius on the right but if you have been here with us awhile you will know there are other causes) and then fix the drift. Do not assume it is the gluteus medius all the time, for if it is not, and you employ more glute medius exercises you could be ignoring the source and building a deeper compensation pattern. Fix the problem, not what you see.
2- Negative foot progression angle and/or internal tibial torsion. In order to fix this you have to know first if you are dealing with a fixed/rigid anatomic tibial or femoral torsion issue which cannot be fixed or if you are dealing with a flexible progression angle issue. Often, “in-toeing” is accompanied with internal tibial torsion, this is because the knee has to progress forward to keep its tracking mechanics clean, if you correct someone’s foot progression back to neutral and they have internal tibial torsion then you have dragged the patellar tracking outside the normal sagittal progression angle, knee pain will ensue. In fact, the foot progression on the ankle is normal, but the tibia or femur are merely torsioned in a manner that drags the foot inwards with the long bone orientation, again, this is driven by a higher order/demand, to normally track the patella sagittally (forward). However, if this is a pre-puberty individual you have time because the long bone derotation process is still occuring. Give homework to encourage a good foot tripod and work to strengthen the external hip rotators and encourage sagittal knee tracking mechanics. This is a delicate balancing act, but it can be done, but it is a monster of a project for a blog post because each case is different, variable and always changing depending on the client progress. Remember, you can only encourage more appropriate mechanics and hope that the body will embrace some of the change and encourage some of the de-rotation process to occur from the long bone growth plates.
The “inside scuff”, to identify its solution you have to know the cause. After all, if it was as easy a fix as “stop doing that” no one would be doing it and we would be out of a job.
Shawn and Ivo …… The Gait Guys
Today we talk about trip and fall incidence, the NFL shoe injury epidemic and so much more ! Join us today on The Gait Guys podcast !
A. Link to our server:
http://thegaitguys.libsyn.com/podcast-40-trips-falls-and-nfl-shoe-injuries
B. iTunes link:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138
C. Gait Guys online /download store (National Shoe Fit Certification and more !) :
http://store.payloadz.com/results/results.aspx?m=80204
D. other web based Gait Guys lectures:
www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
* Today’s show notes:
Neuroscience:




The power to bend bones.
What have we here? Hmmm. This little girl was brought in by her mother because of intermittent knee pain and “collapsing” of the knees while walking, for no apparent reason.
The ankle dorsi flexion (or ankle rocker; see last 2 pictures; we are fully dorsiflexing the ankles) needs to occur somewhere, how about the knees? Or in this case, the tibia. Wow!
You are looking at a 4 year year with a condition called genu (and tibial) recurvatum. Genu recurvatum is operationally defined as knee hyperextension greater than 5 degrees. The knee is hyperextended, and in this case, the tibia is literally “bent backward”. Look at the 2 pictures of her tibia.
Generally speaking, the tibial plateau usually has a slight posterior inclination (as it does in this case; look carefully at the 1st picture) causing the knee to flex slightly when standing. Sometimes, if it is parallel with the ground and the center of gravity is forward of the knees, the knee will hyperextend (or in this case, the tibia will bend) to compensate.
In this particular case, the tibia has compensated more, rather than the knee itself. The knee joint is stable and there is no ligamentous laxity as of yet. She does not have a neurological disorder, neuromuscular disease or connective tissue disorder. She has congenitally tight calves.
As you can imagine, her step length is abbreviated and ankle rocker is impaired.
So what did we tell her Mom?
There you have it. Next time you don’t think Wolff’s (or Davis’s) law* is real, think about this case. Want to know more? Consider taking our National Shoe Fit Program, available by clicking here.
The Gait Guys. Making you gait IQ higher with each post.
*Wolff’s law: Bone will be deposited in areas of stress and removed in areas of strain. or put another way: bone in a healthy person or animal will adapt to the loads under which it is placed
Davis’s law: soft tissue will adapt to the loads that are placed on it


You create your own gait problems.
Just a simple reminder. Most shoes have EVA foam between the hard outsole rubber. EVA foam compresses but it also has memory. If you have a running form issue or a foot type that drives abnormal biomechanics into the shoe then over time the shoe’s EVA foam will break down into that pattern. Not only does this then support the problem, but it enables you to engrain the pattern (which means you are not engraining a cleaner pattern) meaining that every other joint and muscle then assumes that this is the norm and begins to alter their function based on the premise. A sign issue can drive many issues and many other complaints. This client had a rigid rear foot varus , obviously as you can see by the wear pattern (yes, we gently and lovingly flogged this running for wearing the shoes this long into this pattern) but it was made worse by letting the shoe entrench this pattern so deeply. You see, their rear foot varus was no where nearly as bad as the wear into this shoe. But they continued to wear it and the foam continued to break down further and deeper into this varus wedged pattern. They came into see us for lateral knee pain and a tight IT band that was not responding to foam rolling (we immediately began to whimper and then proceeded to thump our forehead into our desk, repeatedly). Some things should be obvious, but even we are far from perfect or wise at times.
Key point, you have heard this here over and over again from us, have 2 or 3 pairs of shoes. Introduce the new shoe into your running repertoire at the 200 mile mark. At that point start rotating your shoes so that you are only a day away from a newer shoe that his not broken down into a faulty pattern and thus deformed EVA foam. Even by the time the one shoe is dead and done, you have not been in it every run. You should never kill a shoe to the 500 mile mark and then buy a new shoe. The pattern you have worn into your shoe will suddenly disappear when you put on the new shoe. Injuries occur from repeated events or sudden changes. Reduce your risk and rotated at least 2 pairs of shoes, one newer and one older.
We talk about alot of these issues, and so much more, in the National Shoe Fit Certification Program. Email us if you think you might be interested. thegaitguys@gmail.com
And ……when it comes to your feet and shoes, use your head.
Shawn and Ivo, The Gait Guys
Video: Wow he just lifted, 232 kg, that is 511 pounds !
What is one of our favorite areas to preach about ? Yes, Ankle dorsiflexion range, or as we often term it, ankle rocker. There are plenty of activities where we need that critical >90degrees (great than) in order to complete the movement at the appropriate joints. Depending on the source you reference and the case by case evaluation, typically 110+ degrees are needed at the ankle hinge mortise (tibiotalar joint) in order to keep the motion from being forced elsewhere. No sport seems to have it as an absolute critical range more than the Clean and Jerk Olympic lift. You can see in this video above, and particularly in this awesome slo-mo video here that we need that magical range in order to do the lift properly.
What will happen if you try to do it with this critical ankle hinge range ? Well, the foot arch can collapse (pronate) to gain more tibial progression and get that tibia to move forward but this will mean that your tibia will be internally spinning which will drag the knee medially and this will create some serious knee loads and patellar tracking issues, to say the very least. Additionally, this spin can risk the anterior hip joint with issues which we will discuss another time.
The body has some pretty strict parameters when it comes to safe loading responses. And if those parameters are not met, then an alternate pattern must be employed if the motion or load must continue. And alternative loads usually lead to pain or injury.
Make sure you have enough ankle range, amongst some other critical parameters, if you are going to lift, especially if you are going to lift heavy. Can you imagine the impacting load on the foot and the ankle if this fella had stiff ankles with less than 110 degrees ankle dorsiflexion ? And remember, merely turning out your feet further doesn’t get you around the problem necessarily. It may help a little, but remember, if you are going to turn your feet out (increase your foot progression angle) the knee tracking has to follow that foot angle, and if it does not, then tibiofemoral torsion will increase and meniscal maceration is a foregone guarantee !
Ankle rocker, it is important stuff. Especially when you are going this big ! But, even if you are doing more remedial squats or Turkish Getups or whatnot.
Shawn and Ivo, The Gait Guys
Can you see the problem in this runner’s gait ?
Trade Secret: Proper Calf Raise
We are selling off part of the farm here today in giving this one away. This is an exercise we prescribe frequently.
When we rise up onto the ball of the foot, most clients and patients tend to come up and either be flush on the forefoot bipod or even a little more onto the lateral aspect of the forefoot. When asked, rarely do we hear that they have a majority of pressure over the medial half of the forefoot. This posturing tendency can lead to inversion sprains. Imagine for a minute a basketball or volleyball player, or any sport for that matter, because most involve the foot leaving the ground and returning to it. When the foot returns to the ground, if the foot is even a slightly bit inverted (meaning they are even slightly tending towards landing on the outer half of the forefoot) an inversion sprain is at risk. This is particularly so when the lateral gastroc-soleus is weak and the peronei are weak. Forefoot valgus foot types are certainly in the risk category here and so once again we find that knowing your foot types so you can help your clients is need-to-know information. Back to our jump and to the return to the ground from the jump, you must remember that the metatarsals are shorter and shorter as you move to the lateral foot. This means that if the load is moving laterally because of posterio-lateral compartment weakness as described above, that the sheer design of the shorter lateral metatarsals will continue to press the motion laterally. This is one of the reasons why lateral ankle strains, inversion sprains, are so frequent and repetitive (we have described the other factor in the latency of the peronei after a single inversion sprain in other blog posts here).
So here we have our calf raise exercise. Squeezing the ball between the ankles on the up (concentric phase) and on the down phase (eccentric) with a nice isometric at the top will force the weight bearing onto the first and second metatarsals (medial forefoot) and drive the lateral compartment to press the motion medially through an isometric instead of depending so much on this compartment to protect the inversion motion through and eccentric. We find this motor pattern terribly weak in our athletes, especially our jumping sports and certainly after inversion sprains. IF we can provide more strength to hold this medial posture during the return to the ground from a jump we can slow or delay the lateral inversion event risk. The key to the exercise is to keep the pressure into the ball medially at all times. A wonderful additional benefit to this exercise is that the user will feel the cocontraction of the thigh adductors which further provides a medial stability effort and blends nicely with the lower abdominals.
You can see that in this case we are rehabilitating an achilles tendon repair case on the left leg.




Footprints in the sand. What do they tell us?
They say that sometimes the silences speak volumes. Take a look at these prints and see if you see the following:
Or, we can comment on what WAS NOT seen:
Just like in the movie “Swordfish”, John Traviolta’s character comments that “It’s all about perception”.
So, what can we surmise from our deductions?
this individual may have a loss of ankle rocker
we are probably looking for someone who has a fore foot varus deformity. This is often accompanied by increased tibial varum
the difference in progression angle may indicate this person has a torsional deformity and/or limited internal rotation of the hips
again, look for someone who has impaired ankle rocker, or limited (at least assymetrical) ankle dorsiflexion
Yes, even when we are on vacation, we are looking at gait, because it is everywhere and affects all forms of human life and behavior.
The Gait Guys. Walking in the sand. Looking for the subtle clues. Teaching you in each and every post
Range of motion that is…..
We can’t tell you how many times we see an aberrant movement pattern or lack of a range of motion during gait (such as ankle rocker or hip extension), only to test them on the table later to find that they have that range of motion available to them, but for some reason they choose to NOT use it.
Yes, range of motion IS very important; but if you have the range and don’t use it; it most certainly will be taken away from you and the resources used elsewhere. You need to know what you are doing and how to do it. Then be able to do it over time, time and time again and finally, able to do it with a load (your body weight +).
Just because you increase someone’s range of motion, does not mean they will be able to incorporate that range of motion into a movement pattern, or compensation pattern for that matter. It is only ¼ of the equation: Range of Motion, Skill (or proprioception), endurance (or the proportion of slow twitch muscle) and strength (the proportion of fast twitch muscle).
Here is an article that supports this notion, by one of our favorite authors; Dr Stu McGill.
The Gait Guys. Taking you to where the rubber meets the road (because some of you are gluten intolerant and therefore separating the wheat from the chaff is not an option).
Moreside, Janice M.1; McGill, Stuart M.2
Abstract: Moreside, JM and McGill, SM. Improvements in hip flexibility do not transfer to mobility in functional movement patterns. J Strength Cond Res 27(10): 2635–2643, 2013—The purpose of this study was to analyze the transference of increased passive hip range of motion (ROM) and core endurance to functional movement. Twenty-four healthy young men with limited hip mobility were randomly assigned to 4 intervention groups: group 1, stretching; group 2, stretching plus hip/spine disassociation exercises; group 3, core endurance; and group 4, control. Previous work has documented the large increase in passive ROM and core endurance that was attained over the 6-week interventions, but whether these changes transferred to functional activities was unclear. Four dynamic activities were analyzed before and after the 6-week interventions: active standing hip extension, lunge, a standing twist/reach maneuver, and exercising on an elliptical trainer. A Vicon motion capture system collected body segment kinematics, with hip and lumbar spine angles subsequently calculated in Visual 3D. Repeated measures analyses of variance determined group effects on various hip and spine angles, with paired t-tests on specific pre/post pairs. Despite the large increases in passive hip ROM, there was no evidence of increased hip ROM used during functional movement testing. Similarly, the only significant change in lumbar motion was a reduction in lumbar rotation during the active hip extension maneuver (p < 0.05). These results indicate that changes in passive ROM or core endurance do not automatically transfer to changes in functional movement patterns. This implies that training and rehabilitation programs may benefit from an additional focus on grooving new motor patterns if newfound movement range is to be used.
It’s that time of the year again….beach cam
With Dr Ivo’s yearly trip to the beach, we have some interesting footage. Today’s winner was this gentleman. We apologize for the shakiness of the camera, as he free handed it for this shot.
Note the following:
As you can see, no one is safe from the gait cam. We are everywhere and the army of gait geeks is growing. Do yourself a favor. Train yourself and others to have ankle rocker, use their glutes to extend their thigh and initiate hip flexion with their abs, rather than the psoas and rectus femoris.
This message is brought to you as a public service by The Gait Guys. Friends don’t let friends have bad biomechanics…


Approaching joint assessment from the perspective of “cylinders”.
Our approach to every joint assessment has long been to visualize and assess the joint(s) as a cylinder since the body parts are cylindrical in form. This has been our approach, and they way we teach, for many years. At each number on the clock (cylinder) there is a theoretical muscle that provides stability to the joint in that vector during loading. The most accurate assessment would be one that investigates the ability of each muscle around the clock (cylinder) to see if it has sufficient S.E.S. (Skill, Endurance, Strength) as well as how well that muscle(s) participates with the synergists, antagonists and agonists (ie. motor patterns for stability and mobility). We do this at each joint along the kinetic chain when assessing someone with a clinical or functional problem.
When dealing with a frontal plane drift, as in the 3rd photo above where you see the person’s (black shorts) pelvis drift laterally outside the perpendicular foot line, one could naturally assume that the gluteus medius is weak (9 o'clock) but the wise clinician would also look at the other side of that cylinder to see if the adductors were involved (3 o'clock) since that is 180 degrees through the joint axis. (Note: Runners are sagittal athletes so frontal plane weaknesses are often seen. This is not desirable however, this is a perfect example why runners should cross train more into lateral and angular sports to ensure that the sagittal plane does not dominate.) Obviously the foot and the knee also need a similar cylindrical assessment approach. We have spoken loudly many times here and on our podcasts over the years that quite often there are multiple flaws in a presentation, typically a focal cause and one if not several compensations as a functional adaptation strategy around that central flaw. In this runner’s case there could be medial knee weakness or foot weaknesses that are affording too much medial drift and spin of the limb resulting in the lateral pelvic drift compensation. But, just because the gluteus medius shows up weak does not mean that it is the focal point of clinical intervention. If one facilitates the gluteus medius and does not address the causative lower cylinder issues then they are quite possibly empowering the compensation and enabling the aberrant activity to continue. Knowingly or unknowingly layering armor or inappropriate strength to a pathologic compensation pattern at a focal joint level that is not the focal cause should be a clinical crime, but it is done every day by people who do not know better even though their efforts are well intended.
Ok, we got on a bit of a soap box rant there, sorry. Back to the case at hand.
Your assessment should not stop at the frontal plane in this case. If there is an imbalance in the sagittal plane in this sagittal athlete this can be a causative problem as well, which is why the cylinder approach should not stop at the frontal plane or when you find that first major weakness. In frontal pelvic drift cases, there is quite often an anterior pelvic tilt where the lower abdominals can be weak, the low back is slightly extended and the paraspinals are more active. This is the classic “impaired hip extension pattern” and sets up a Janda/Lewitt style “Layered Syndrome”. Most of the time, resolving this sagittal flaw will show immediate improvement of the frontal plane deficits. But, do not think it is as simple as re-facilitating these 2 patterns. Remember, neuromotor reprogramming and patterning takes 8-12 weeks by some sources. And remember, the initial strength gains in the first few weeks are from neuroadaptation (ie, skill gains in coordination), these gains are not the true physiological endurance and strength gains that we desire for an athlete. Those gains take time but they are the ones that we need for sport performance and joint power.
And then there is the rotational or axial component, which we did not even begin to discuss here. We have briefly talked about the frontal and sagittal cylinder aspects, and yes, we have just skimmed the surface as there are multiple patterns and issues which we have had to leave out here so that this doesn’t turn into a full fledged chapter for our next book. This stuff gets complicated and can leave you running in mental circles at times. But these concepts will help you better understand why you often see neuro-protective tightness 180 degrees on the other side of the cylinder from tightness, and when you address the weakness the other side of the cylinder some of that neuro-protective tone is eased. But again, it is not nearly this simple because you must remember that if your assessment is static or on a table then your findings will be functionally imprecise. And, not stopping there, there are multiple joints below the joint you are focusing on, and multiple joint complexes above as well. Plus, there are 3 other limbs that can play into the function and dysfunction of a given limb and its joints. There are breathing patterns, postural patterns and many other issues. This is not an easy game to play, let alone play it well or wisely for your athlete.
In today’s photos we wanted to show you 3 runners. One a distance runner with good joint stacking and one sprinter with amazing joint stacking. And then the runner in the black shorts, who cannot stack the foot, knee or hips even remotely well. This runner in the back shorts will have the cross over gait and likely have the medial ankle scuff marks to prove it. But remember, there is one component that we often talk about, one we did not discuss here … . . are there also torsional issues in this runner ? Do they have femoral or tibial torsion(s) ? What is their foot type ? Are they in the right shoe for their foot type ? Are some of these components playing into their visibly flawed mechanics ?
Below is an article we have put up here on the blog previously. It is a study where the investigators examined hip abductor strength (watch this video here ) in distance runners with iliotibial band syndrome comparing injured limb strength to the unaffected limb to determine whether correction of the strength deficits in the HAM’s (hip abductor muscles) correlates with successful outcomes. The study showed the obvious, that runners with ITBS have weaker HAM strength compared to the asymptomatic leg.
But here is our question, did they just strengthen the compensation for an apparently successful outcome, or did they address the problem ? Only time will tell if you actually fixed something or merely enabled the dysfunctional motor pattern by layering it with more armor for the next battle. If it is fixed the problem and all of its associated problems should go away. But if the runner comes back weeks later with knee complaints, foot pain, back pain or the like … . . then the message should be loud and clear.
Shawn and Ivo, The Gait Guys……today with soap on the bottom of our feet.
References:
Clin J Sport Med. 2000 Jul;10(3):169-75. Hip abductor weakness in distance runners with iliotibial band syndrome. Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N,Sahrmann SA. Department of Functional Restoration, Stanford University, California 94305-5105, USA.
A. Link to our server:
http://thegaitguys.libsyn.com/podcast-39-ankle-mobilizations-plyos-bunions
B. iTunes link:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138
C. Gait Guys online /download store (National Shoe Fit Certification and more !) :
http://store.payloadz.com/results/results.aspx?m=80204
D. other web based Gait Guys lectures:
www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
* Today’s show notes:
The Case of the Non Rotating Knee
Here is a runner, wanting to be an ultra runner, who recently developed right sided knee pain while running a 50K. He was pacing another individual and developed pain on the outside (lateral patella and knee) on the right, ascending and especially descending hills. The pain is dull and achy. He is able to “push through” the pain, but if he does, it remains painful for a few days.
He has an anatomically short leg on the L (tibial). There is no significant tibial torsion (he has normal external version) and not femoral torsion. There are adequate amounts of internal (>15 degrees) and external (>30 degrees) rotation of the hips.
He has 7 degrees ankle dorsiflexion on the right, 10 degrees on the left. On the table (and in the video) he has 0 degrees of hip extension during passive motion, walking and running. He has weakness of the long extensors of the toes, as well as the abductors.
Take a look at his video. Note the following:
· the right knee has less medial excursion than the left (watch the dots)
· rearfoot valgus is noted on the L (ie. calcaneus is everted)
· subtle lean to Left on L sided stance phase
· when barefoot, the problem lessens
Why does the right knee rotate less than the left?
When folks have a short leg, we generally expect that leg to remain in supination (thus external rotation) more and the longer leg to internally rotate more, due to excessive pronation. But here, we see the opposite. You will notice he has a rearfoot valgus on the left. This means the midtarsal joint is in a greater amount of pronation on the shorter side. For every action, there is an equal and opposite reaction. In this case, less pronation (or supination) on the longer leg side. Remember, we said generally folks pronate more on the long leg side. This is one of the exceptions.
So, should he throw away his shoes?
The shoes, which have a certain amount of torsional rigidity, are compounding the problem. The Brooks Cascadia is an excellent trail running shoe, he just needs something with less torsional rigidity. the shoe does not allow his knee to come midline sufficiently. Since he is a Brooks Fan, we suggested the “Grit” in the Pure line. 4mm drop and less rigid torsionally. He could also work his way into a “Drift” (4mm or zero drop, extremely flexible).
Why does he lean to the left on stance phase on the left?
Most likely, to clear the right long leg on swing phase. This is one of the 5 common strategies. For more strategies, click here.
Why is it better when he is barefoot? It must mean he should be a barefoot runner, right?
He is better, because there is less impediment to the foot pronating (ie. the shoe has less torsional rigidity)
The Gait Guys. Making you a better diagnostician, with each and every post.
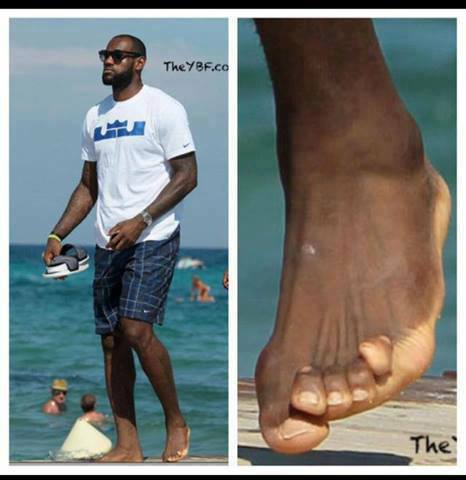
http://bleacherreport.com/articles/1757693-everybody-look-at-lebron-james-toes
This is what happens when you get too much short extensor tone and/or strength in the digits of the foot. Now this is his trailing foot and he has moved into toe off so he should be activating his toe extensors and the tibialis anterior (ie. the anterior compartment) to create clearance for that foot so that he doesn’t catch the toes on the swing through phase of gait. In this case we do not see alot of ankle dorsiflexion (which we should see at this point) so we are seeing a compensation of perhaps increased short extensor (of the toes) activity.
We also see what appears to be a drifting of the big toe (the hallux) underneath the 2nd toe. This often happens when a bunion or hallux valgus is present. Now we do not see a bunion present here but the viewing angle is not optimal however it does appear that there is a slight drift of the hallux big toe towards the lesser toes . We are not sure if we would qualify this as hallux valgus, and if so it is mild, but none the less we see a slight lateral drift. What is interesting is that despite the obvious activity of the lesser toes short extensor muscle (EDB) we do not see a simultaneous activity of the short extensor of the hallux (EHB, extensor hallucis brevis). Does he need to do our exercise ? See video link here !
And so, when the lesser toes are in extension as we see here and the big toe is not moving into extension, and when that is simultaneously combined with even a little hallux valgus tendency, the big toe will drift underneath the lesser toes as we see here, even appearing to push the 2nd toe further into extension.
As for his little toe, well, Dr. Allen has one just like it so perhaps he missed his calling in the NBA. Some folks just do not have as plantarward orientation of the 5th toe and so it migrates upward (dorsally) a little. This can be from birth but it can also come from trauma. But in time because the toe is not more plantar oriented, the dorsal muscles (the extensors) become more dominant and the toe just starts to take on this kind of appearance and orientation. It will reduce significantly when the foot is on the ground and the extensors are turned off, but it looks more shocking during the swing phase because of the extensor dominance in that phase.
This kind of presentation if left unchecked can lead to hammer toes, plantar fat pad migration distally exposing the metatarsal heads to more plantar forces without protection and a host of other problems. Lebron needs to do our Shuffle Walk Exercise to get more ankle rocker (dorsiflexion) and also work to increase his long toe extensors (EDL) and lumbricals. This will flatten his toes and improve mechanical leverage. Remember, if you gait better foot function with increased ankle dorsiflexion you will get more hip extension and more glute function. But does the big fella really need to jump any higher? We are sure he would accept being faster though … . who wouldn’t ?
Fee for today’s long distance consult: … Lebron, lets say 10,000$ and we will call it even. Sound good ? But a lifetime of prettier, stronger and more functional toes……priceless. Have your people contact our people. (Ok, we don’t have people, but we do have an email address here on our blog !).
Shawn and Ivo, The Gait Guys. Even helping the elite, little by little.
Our show notes should interest you today. We have another great podcast ready for you !
Link to our server:
http://thegaitguys.libsyn.com/podcast-38-usain-bolt-arm-swing-ballasts-running-stuff
iTunes link:
https://itunes.apple.com/us/podcast/the-gait-guys-podcast/id559864138
Gait Guys online /download store (National Shoe Fit Certification and more !) :
http://store.payloadz.com/results/results.aspx?m=80204
other web based Gait Guys lectures:
www.onlinece.com type in Dr. Waerlop or Dr. Allen, ”Biomechanics”
Today’s show notes:
Rehabilitation Neuroscience Laboratory, University of Victoria, BC, Canada. pzehr@uvic.ca
Abstract: Walking can be a very automated process, and it is likely that central pattern generators (CPGs) play a role in the coordination of the limbs. Recent evidence suggests that both the arms and legs are regulated by CPGs and that sensory feedback also regulates the CPG activity and assists in mediating interlimb coordination. Although the strength of coupling between the legs is stronger than that between the arms, arm and leg movements are similarly regulated by CPG activity and sensory feedback (e.g., reflex control) during locomotion
A recent study cited in Competitor Magazine, talked about common stride “improvements” actually may reduce running economy. They looked at stride rate (cadence) and vertical displacement. One would think, with all the hoopla out there, that more steps per minute and less vertical displacement would be more efficient. The actual study concluded “Alterations led to an increase in metabolic cost in most cases, measured as VO2 uptake per minute and kg body mass,” Another study which had similar results can be found here.
Even though the study had a small sample size (16 participants), If you think about this, it makes sense. Volitional effort usually has a metabolic cost. It does not make it right or wrong; they are just the facts. The nervous system will take time to integrate new (motor) patterns. Each person has a optimal (homestatic) stride “style” which includes vertical displacement as well as stride length, among other factors (lateral sway, ankle dorsi pantar flexion, knee flexion, thigh flexion, etc).
The study itself also concluded ““Mid- and long-term effects of altering … technique should also be studied.” we concur, we have not seen any long term studies that look at economy over time, but would love to read them if any of our readers run across them.
The Gait Guys. Bringing you the facts without the bling.

Donate here











Help keep us free ! Make a donation by clicking. here.

Donate to get exclusive content from The Gait Guys
OUR SEARCH BOX IS INTUITIVE, TYPE IN YOUR KEY WORD, WAIT, THEN SCROLL DOWN.
Email us: our email is found under the "Disclaimer" Tab above.

Powered by Squarespace.