

The Foot Tripod; Part 2
Here we go. More stuff you can use today. Pay attention to the subtleties of this simple, yet effective exercise we use on a daily basis.
Have a great Friday
Ivo and Shawn
The Foot Tripod; Part 2
Here we go. More stuff you can use today. Pay attention to the subtleties of this simple, yet effective exercise we use on a daily basis.
Have a great Friday
Ivo and Shawn

Here is an oldie but a goodie.
The Flash ! A return to concepts of heel strike, hamstrings and abdominals. This was from our first steps into blogging. Enjoy.
http://thegaitguys.tumblr.com/post/3902070321/more-gait-guy-gait-gaffs-what-it-would-look-like
here is the link for podcast 13
http://thegaitguys.libsyn.com/webpage
______________________________
1- Malcolm gladwells piece on drug doping (PEDs) in sports:
“Gladwell argued that we should think about cycling the same way we think about auto racing — where teams should be rewarded for using science and bending the rules to their breaking point to succeed.
"When you look at what Lance is alleged to have done. Basically he was better than everyone else at using PEDs,” Gladwell said. “He was the guy who sat down and was rigorous and focused and thoughtful and intelligent and cutting edge in how to use them, and apply them and make himself better. Like, I don’t know, so is that a bad thing?”
Read more: http://www.businessinsider.com/malcolm-gladwell-lance-armstrong-2012-10#ixzz29QBKJpAJ
2- Caffeine: A PED ?
Mens health online magazine, also found in our Sunday edition Oct 14th, 2012 newspaper:
http://news.menshealth.com/chew-gum-before-races/2012/04/12/
Chew on this: Caffeinated gum can improve your athletic performance—if you start chewing it at the right moment, finds a new study from Kent State University.
NICOTINE: http://www.t-nation.com/free_online_article/most_recent/50_hits_of_nicotine
Nicotine has been used in energy drinks in Japan for years.
stimulates the release of acetylcholine, providing a sense of increased energy. Arnold used to do commercials for them.
Nicotine can improve reaction time.
Nicotine can be addictive, much like caffeine. But addiction to nicotine gum, lozenges, or patches is rare, if not unheard of.
MAYO clinic: http://www.mayoclinic.org/medical-edge-newspaper-2009/apr-24b.html
3- DISCLAIMER:We are not your doctors so anything you hear here should not be taken as medical advice. For that you need to visit YOUR doctors and ask them the questions. We have not examined you, we do not know you, we know very little about your medical status. So, do not hold us responsible for taking our advice when we have just told you not to ! Again, we are NOT your doctors !
4: Maryland Guy Running a marathon in flip flops:
“Some of the rules: It can’t be a heal strap. There can’t be any other means to hold the flip flop on your shoe besides just the normal thing between your toes,” Levasseur said. “I don’t know what happens if I get a blowout.”
Read more: http://www.wbaltv.com/news/sports/Man-to-run-Baltimore-marathon-in-flip-flops/-/9379464/16917220/-/remeou/-/index.html#ixzz29QDIyW4d
5-Managing Ankle Sprains:
http://www.running-physio.com/anklesprain/
6- HIIT
http://www.the15minutes.info/2012/10/12/what-is-hiit-and-what-can-it-do-for-you/
http://sportsmedicine.about.com/od/anatomyandphysiology/a/Deconditioning.htm
Studies have shown that you can maintain your fitness level even if you need to change or cut back on you exercise for several months. In order to do so, you need to exercise at about 70 percent of your VO2 max at least once per week.
7- EMAIL FROM A Blog follower:
middleagedathlete asked you:
I searched the site and didn’t see anything on bow-leggedness (if that’s a word) and it’s impact on gait. I have mild to moderate bow legs and never even knew it until I started running and it was pointed out to me by a PT I was seeing for knee pain. Is there an optimal (or at a minimum least bad) strategy for running with bow legs? I am 6'0" tall and have a gap of about 2" between my knees when standing with my ankles together and my legs straight. I am curious to hear your thoughts.
8- from the newspaper:
from Barefoot Running University.com
Article: Running up Hill
http://barefootrunninguniversity.com/2012/10/12/uphill-running-technique/
9- Blog post we liked recently: October 5th, Gait Running and Sound. Are you listening to your body ?
10- Random topic: Wednesday october 10th Peter larson who runs Runblogger did a review of the following article:
Minimalist Running Results in Fewer Injuries?: Survey Suggests that Traditionally Shod Runners are 3.41 Times More Likely to Get Hurt
we have not gotten through the research article yet but we will, and we will try to address out thoughts on it and pete’s in the next 1-2 podcasts. We want to make sure our thoughts are heard as well. We bet Pete did a phenomenal job but we like to see things for ourselves, just like pete does. He is a stickler to details like we are, which is why we like alot of his work. So, stay tuned !
11- Our dvd’s and efile downloads
Are all on payloadz. Link is in the show notes.
Link: http://store.payloadz.com/results/results.asp?m=80204
Every now and then we come across something that we think the whole world should know about, kind of like GMO foods. Gluten is another. Today, more than 1 in 133 Americans suffer from gluten related health problems while an even higher percentage of the population goes undiagnosed with an emerging condition called ‘gluten sensitivity.’ From a website doctorauer.com we discovered, but have not yet fact checked this following historical mention:
“In 1843, a physician named Stanislas Tanchou spoke at the Paris Medical Society Conference. He claimed that he could predict the cancer rates in major European cities over the next 50 years. He based his predictions on the percentage of grains being consumed in each major city. What is astonishing is that, over time, his predictions turned out to be correct. In the cities that had the highest grain consumption, cancer rates were the highest. This is in stark contrast to the fact that in populations who did not consume grains, cancer did not exist." - article link
Here at The Gait Guys, being doctors who treat athletes and non-athletes, we have written about gluten in previous blog posts on "Gluten Ataxia” (Link) and Running yourself into Hormone Trouble (link) because we felt it was important to spread the wisdom. We even recently talked about gluten and how it can damage your thyroid profile and gut via one of the gluten subfractions called gliadin on podcast #12 (link).
These dialogues seemed to spur one of our brilliant and engaged readers and listeners. Jim sent us a series of emails which you will find below. We obtained his permission to reproduce the emails (thx Jim !). We will also welcome him to chime in further on Facebook when this post cross-links if he has further input.
We are building a wonderful and brilliant readership and fast growing podcast following. We have smart folks joining the brethren here at The Gait Guys ! And we are blessed to have Jim, and celebrate his homework and knowledge here.
Everyone should read this, especially if you have tested gluten insensitive but still have gut issues or immune issues. You may have your eyes opened !
PS * at the very bottom of this blog post you will find a link to a wonderful video youtube lecture by Dr Osborne. If you watch the first 4 minutes you will learn that corn, millet, oats, rice, rye, sorgum and barley all have their own types of gluten in them. You will clearly understand why a sensitive person MIGHT get away with rice but not wheat. Hence why this is a very difficult problem for the average consumer.
Thanks Jim !
_______________________________
Greetings Gait Guys!
In Nora Gedgadaus’ book “Primal Body, Primal Mind”, she explains that there are actually 12 subfractions of the gliadin protein (gliadin is a biproduct of gluten metabolism). According to her, at least at the time she wrote the book (2012 or 2011) there was only one lab in existence that could test for all 12 subfractions: Cyrex Labs. Most of the other labs only test for the “alpha” subfraction. This is why there are so many false negatives. But the best way is just to go by how one reacts individually to it. For some reason, science doesn’t trump nature as some would have us believe…
“Grains are truly humanity’s double edged sword. They enabled us to leave behind our hunter gatherer lifestyle and created the foundation for the modern societies as we know them today. On the other hand, there is growing evidence that they are one of the major culprits for our health problems.
We must remember that evolutionarily speaking, we have been around for almost two million years, but we have only been eating grains for a few thousand. As such, our bodies have not had the time to adapt to this “new” food in our diet. Furthermore, modern farming, harvesting, and processing methods have stripped grains of their nutritional integrity, decreasing their digestibility, and making them highly toxic and inflammatory food to our bodies. With no doubt, today’s grains are proving to be one of the major underlying contributors to the development of degenerative diseases as we known them today.”
Byron Richards websites are http://www.wellnessresources.com/ and http://www.byronrichards.com/ .

Another IFGEC Certified! Eric is our 1st non retail individual to pass the exam!
Some comments on the course an exam from Eric:
“ I was impressed by the depth of the material and your abilities to keep a highly complex subject like foot/ankle mechanics and shoe fit to only 3 hours. I have been to a full weekend course on the foot/ankle and didn’t leave with as much practical knowledge! As for the exam, I noticed that some questions had a couple of layers to them that really ensured that the material presented needed to be understood by the participant. I haven’t taken a test before where I received immediate feedback on whether I was right or wrong. At times, I got a little too excited at knowing I was wrong, but for the most part that may help people take extra time to think their answers through.
As for studying, everyone is different. I watched the video three times, took detailed notes and studied them. Also, I’ve been an avid follower of the blog, facebook page and now podcast since I saw Dr. Allen present for the NSCA earlier this year at Chicago State University.
I am the manager for an outpatient orthopedic facility in Flossmoor, IL (southern suburb of Chicago). The overwhelming majority of referrals are worker comp physical therapy and work conditioning patients. I primarily took the course to answer my and my patient’s questions on proper shoe choice and since I’m not a runner, I really didn’t put much thought into shoes beyond "whatever feels comfortable." I have much more confidence on what recommendations need to be made following this course.”
The Gait Guys. Stepping toward foot, gait and shoe competency, one individual at a time
Welcome to Friday Follies, Folks.
Amidst one of our many forays into cyberspace, we came upon this: Mr Potato-rthotic.
Have a great weekend!
Ivo and Shawn
Do you have enough Ankle Dorsiflexion to do this ? Some clues ?
Two guys pulling 40,000 pounds over one mile in just over an hour !
Watch the video above and then check out this link.
http://www.powerropes.com/brtrophy.html
Look at the fellas left foot in the video compared to his right. Notice the turn out (the increased progression angle as it is referred to as) ? Now look at the photos from the article link above, again the fella in the red shirt has his left foot turned out again. Why is he doing this ?
Because he does not likely have enough ankle dorsiflexion (ankle rocker) to get into this far of a forward lean. Have you seen this in people or your students doing squats ? Lunges ? Will this present in his normal gait ? Perhaps, but if he has enough for normal gait (~15 degrees past vertical 90 degrees) he shouldn’t need to turn it out.
Turning out the foot will allow you to pronate through the midfoot to gain more dorsiflexion. It is why some people do it. Look for it.
It is also possible that he has a painful big toe or a hallux rigidus/limitus (ie. turn toe) and thus cannot toe off sagittally like on the other foot or like the other fella. This turn out will avoid loading that joint as much.
Regardless, you must examine this fella and figure out why he is using this strategy only on one side. This is just one theory, but we did not want to pollute this post with a few others. We can do that another time.
Ankle rocker dorsiflexion. It is critical for some activities.
Shawn and Ivo
__________
from a FAcebook reader:

Hi Gait Guys gang:
Some temporary changes as we move into Q4 of the year. The Gait Guys have some big projects on our desk. Things we want to get done for you, our loyal followers. We have some new additions and directions for the podcast which you will all likely enjoy, especially those of you who feel that the info is a bit too complex at times with too much medical and latin jargon. We will be skipping a podcast this week to ready ourselves for the change.
But being the busiest time of the year for us in our clinics, plus holidays coming soon, we will be doing only 2-3 blog posts per week now so we can get the other projects done for you by the end of the year. You will likely hardly notice the change as other things come aboard, but we wanted you to know we are not going anywhere, or losing steam in our mission. Time is just our most precious commodity and we are a bit short on it in Q4. Enjoy today’s blog post on Part 3 of the Frontal Plane Hip Biomechanics. 3 down, and 3 more parts to go !
Shawn and Ivo
Hip Biomechanics: Frontal Plane Part 3
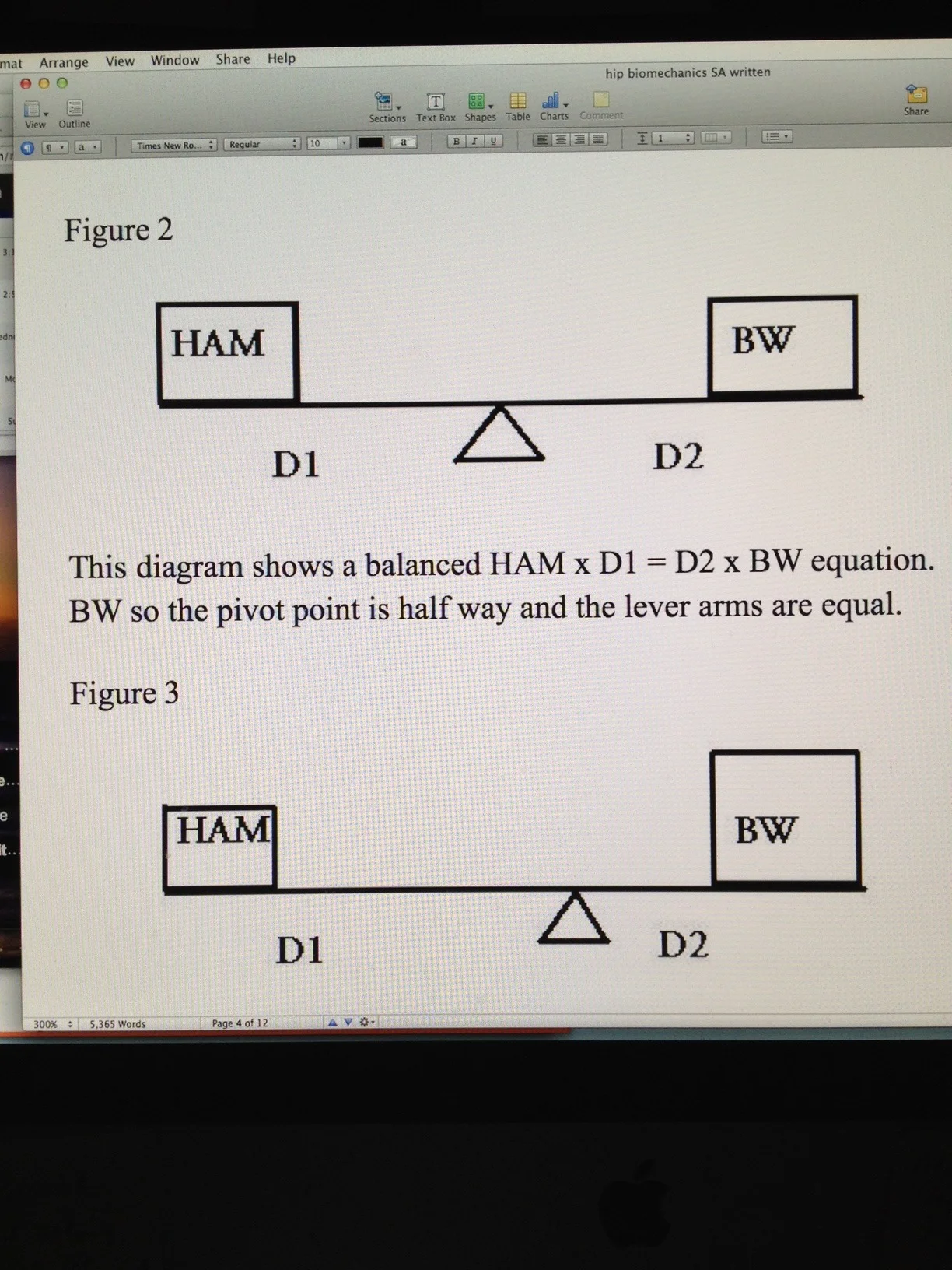
This diagram (Figure 3) also shows a balanced HAM x D1 = D2 x BW equation. The BW is larger than the HAM but this is offset in the rules of the teeter-totter. Shifting the pivot point towards the larger mass is offset by the smaller D2 and larger D1 moment arms. This is a typical compensatory mechanism used by obese patients to ambulate effectively. It does render significant frontal plane movement of the pelvis instead of the more desirable silent frontal plane pelvis. In this compensation, even large body weights can be somewhat offset by the degree of contralateral hip hiking to reduce the D2 moment arm and increase the D1 moment arm however this compensation has its limits. When the limits of alteration of moment arm length are reached the body’s only compensation at that point is to increase the HAM forces which increases joint compression and thus cartilage wear since the cyclical loading and unloading of the cartilage is much less. This is also the same mechanism used by patients with a osteoarthritic painful hip joint. We are not referring to increasing BW, rather we are suggesting that to reduce pain the patient will want less joint compression and thus a reduced HAM. To do this we want to increase the D1 moment arm. The only way other than surgery to achieve this increase in D1 is to take the existing body weight and shift it closer to the pivot point. Ideally you would want to lean so far over the affected painful hip as to get your body weight (BW) immediately over the pivot point. This is what is done with a walking cane in the opposite hand of the stance leg, to help lift the swing phase leg and pelvis and to push the body mass over the hip WITHOUT using more HAM (glute medius contraction generated compression, which would generate pain). This would effectively reduce D2 to nil and significantly increase D1 thus allowing HAM to be minimal; thus reducing painful joint compression. (In teeter-totter verbiage, put the small child on the long part of the teeter-totter arm and you can move large forces with little effort at the pivot point.)

Get Certified!
Our 2nd Nationally Certified Individual! Congratulations to Marianne Fitzgerald, LMT. Marianne is the coordinator of “ all things shoes and sox” @ Summit Chiropractic Rehabilitation, PC in Dillon, Colorado ( Dr Ivo’s office).
“The course was super informative and well structured. It was great to be able to watch the videos online at my own pace and on my schedule. I learn by repetition so I was able to watch each one a couple of times. . The exam was challenging but no trick questions. I wish I had taken better notes because I know that all the information on the test was in the video. Now when I’m working with someone to try on shoes and hopefully buy them, I feel more confident and actually sound like I know what I’m talking about.”
The Gait Guys: spreading gait, foot and shoe competency, one pair at a time…

A Tale of Two Footies
Time for a pedograph, folks. What do we have here? Look at the last analysis here.
To review :
Let’s divide the foot into 3 sections: the rear foot, the mid foot and the fore foot.
First of all, are they symmetrical? Look carefully at the fore foot on each side. NO! the right foot looks different than the left, so we are looking at asymmetrical pathology.
Let’s start at the rear foot: The heel teardrop is elongated on both sides, slightly more on the right; this means incraesed calcaneal eversion (or rearfoot pronation) bilaterally, R > L. The right heel shows increased pressure (more ink = more pressure).
Next up, the mid foot. Similar shapes, more pressure and printing on the left. Did you notice the “tail” of the 5th metatarsal printing, giving it a wider print? This person is staying on the outside of their foot longer than normal, right (more ink) more than left.
How about the fore foot? Lots going on there.
Lets start on the left
Notice the mild increased printing of the 5th and 4th metatarsal heads. Force should be traveling from lateral to medial here, as the foot goes into supination. A relatively normal amount of pressure on the head of the 1st metatarsal.
Now look at the toes. Notice that space between the 2nd and 3rd? This gal had an old fracture and has an increased space between them.
Now how about the right?
Increased pressure on most of the heads with a concentration on the 1st metatarsal. Hmmm…what would cause that? this is typical of someone who has a 1st ray (cunieform and metatarsal) that is hypomobile, such as with someone with a forefoot valgus (as this person does) or a dropped 1st metatarsal head (which is usually rigid, as is NOT the case here).
Did you see that rpinting at the medial aspect of the proximal phalanyx of the hallux (ie. big toe)? This gal externally rotates the lower extremity to push off the big toe to propel herself forward. This is because the 1st metatarsal head hits the ground BEFORE the 5th (as we would normally expect to see, like in the left foot), and because the weight is now on the outside of the foot, she need to push off SOMETHING.
Getting better at this? We hope so. Keep reading the blog and look at some of our past pedograph posts here.
The Gait Guys. Teaching you about the importance of gait, each and every day!
here is the PODCAST link and show notes. You can also find us on iTunes:
http://thegaitguys.libsyn.com/webpage
and here on iTunes (click)
______________________________
Payloadz link for our DVD’s and efile downloads: http://store.payloadz.com/results/results.asp?m=80204
1- Email from our New Newspaper “the Gait guys daily”:
“What do to when you cannot run.” - Triathlon.Competitor.com
link: http://triathlon.competitor.com/2012/10/training/what-to-do-when-you-cant-run_63237
Research suggests that nearly half of all runners experience an injury every year. That’s a whole lot runners sentenced to time off
- so many runners want to still run……Alter G treadmill, pool running
-there are a number of workout alternatives that allow you time to heal without sending you back to square one of your training regimen.
- maintain general fitness, while also providing an important psychological boost
- rowing, nordic ski, swimming, skating (slide boards)
- lateral plane sports for glutes and ankle stability
- reduce injury
2- Winter running on ice……another article on our newspaper:
http://www.outsideonline.com/outdoor-gear/gear-guy/The-Best-Running-Solution-for-Icy-Roads-DIY-Sheet-Metal-Screws.html
sheet metal screws
yaktrax
Kohtoola Microspikes,
32 North Stabilicers Sport,
http://icespike.net/ “ICESPIKE™ is like sheet metal screws on STEROIDS
3- DISCLAIMER:
We are not your doctors so anything you hear here should not be taken as medical advice. For that you need to visit YOUR doctors and ask them the questions. We have not examined you, we do not know you, we know very little about your medical status. So, do not hold us responsible for taking our advice when we have just told you not to ! Again, we are NOT your doctors !
4- Updates and Sponsor talk:
A- more lectures available on www.onlineCE.com Go there and look up our lectures
B- In January we will be taking on sponsors for our podcast. We have had some interest already but we wanted to work out the quality control issues first. Early in means savings.
Contact us if you would like to be a sponsor……If we believe your product has value to this listener community we will give you a professional and personalized company or product plug and advertisment. From our lips to our listeners ears !
We will basically expose your product to our international fan base.
The sponsors will help make our mission possible, defray costs and time to put out this podcast and blog. These things take is away from our practices a little. Each week we will have 2 center-Stage sponsors . Your sponsorship can run as long as you want.
6- Blog READER EMAIL:
5- EMAIL FROM A Blog follower:
Hi Gait Guys,First of all I really enjoy reading your posts and watching the Youtube clips. They have really helped me in my work.I have a small question for you if you don’t mind me asking. I’ve noticed on a number of running gait assessments that when viewing from the back the whole foot moves medially whilst the forefoot rotates outwards in some individuals. The knee also moves out to and looks like the hip is externally rotating.I presume this is not normal (i may be wrong) as the leg needs to recover in a straight line.My question is why does this happen and if it’s not normal how do you correct it?I’ve attached a small video for viewing.I look forward to hearing from you.Kind regards, DAVID
7- Our dvd’s and efile downloads
Are all on payloadz. Link is in the show notes.
Link: http://store.payloadz.com/results/results.asp?m=80204
8 - Email from a Blog Reader
9- From a blog reader:
jdawg70 asked us a questions on our tumblr blog page
I think I have external tibial torsion on the right with a dropped arch on that foot and front of hip and groin pain on the left leg. I have had standing x-rays of my pelvis from the chiropractor showing a difference in hip heights of 9mm from left to right, that is, the left being that much higher. I do have lots of pain and digestive problems. I was hoping you could help or advise me. I highly value your opinions
10- From one of our Blog readers who contacted us through the blog:
My name is Maury. Two years ago I noticed my left foot turning out all the time -walking, standing, exercising, etc. I also had hip pain. Eventually we discovered a labral tear and a torn ligamentum teres in the left hip. I had the repair done arthroscopically February 1st, 2012. It is now August and I am still experiencing the hip/foot turned out. My rotation/mobility/flexibility is fairly equal on both sides. My strength is good. I am at a loss. What can I do about this? Thank you.
11- From another blog reader:
from Sherryb1 on the blog
I think there is a correlation between adducted toes–especially adducted and flexed ip joint toes and abdominal strength/weakness. When balance is difficult, you can usually spot the adducted and flexed IP toes. When you watch someone walking with a little balance inefficiency, often you will find adducted and flexed IP toes. Do you see it as the chicken or the egg? Belly/toes, or toes/belly. And have you seen this and, might you have seen anything in the literature to substantiate it? Thank you

Hip Biomechanics Part 2
Figure 1 shows the condensed version of the parameters (forces and moment arms) affecting movement and stability of the femur-acetabulum complex in the frontal plane during the closed kinetic chain. (A moment arm such as D1 and D2 is defined as the length of a line that extends from the axis of rotation to a point of right angle intersection with a respective force, in this case HAM or BW.)
In Figure 1 above we see several parameters. HAM represents the Hip Abductor Muscles, D1 represents the internal moment arm, D2 represents the external moment arm and BW represents the Body Weight of the individual. These factors all come into play when considering the frontal plane equilibrium of the hip joint. The equation representing the interaction of all of these parameters is HAM x D1 = D2 x BW. Both sides of this equation must be equal and balanced in order for the pelvis to remain stable and without movement when in the closed chain stance phase of gait. In this diagram, if the left side of the equation is greater than the right the net effect will be a counterclockwise hip moment and the patient will move their torso over the hip creating a hiking or lifting of the contralateral hip. This net movement will create abduction at the hip joint. If the right side of the equation is greater than the left the net effect will be a clockwise hip moment and the patient will move their torso away from the hip creating a dropping of the contralateral hip. This net movement will create adduction at the hip joint seen here and thus the classic Trendelenberg gait. We need to keep in mind that this is not a perfect model presented here since we are ignoring acceleration of the body in the forward sagittal plane and rotational planes. Investigating the equation further should bring the reader to further realization that if the body weight (BW) were to increase, mathematically the D2 external moment arm could decrease to keep the equation balanced. However, since the length of this D2 moment arm is rather fixed (unless the pelvis were to go through a counterclockwise rotation which would draw the body weight center closer to the hip joint center effectually abducting the stance hip, thus reducing the D2 moment arm) this is not a more likely scenario. Rather, the response would be to attempt to increase the left side of the mathematical equation thus increasing the HAM forces to attempt to keep the pelvis level and the equation from changing. In other words, when body weight increases we must increase the gain or contraction in the HAM group during each step to keep the pelvis level and balanced. Unfortunately the HAM strength has its limits of maximal contraction, sometimes far below any major increases in body weight. One must keep in mind that with increased HAM contraction there is a corresponding increase in joint compression across the hip articular surfaces which at reasonable levels is well embraced but at unreasonable levels can damage articular cartilage. One should thus conclude that maintaining a reasonable body weight for one’s bone structure keeps the right and left sides of the mathematical equation at tolerable levels, both for movement, stability and cartilage longevity. Fortunately the equation has a built in safety mechanism for these counterclockwise hip moments, one that is beneficial. In such scenarios, as the body is brought over the hip thus decreasing the D2 moment arm, the D1-internal moment arm increases in length and since the equation must be balanced the HAM force can decrease. Thus, the magnitude of the HAM force is inversely proportional to the length of the D1-internal moment arm. The whole equation can better be visualized and conceptualized by a teeter totter diagram with a sliding pivot point.
Shawn and Ivo, The Gait (and biomechanics) Guys
Hip Biomechanics
The following excerpted text is copywrited from the textbook; “Form and Function: The Scientific Basis of Movement and Movement Impairment” (Dr. S. Allen, Dr. E. Osar)
Frontal Plane Functional Biomechanics
The hip is a very complex joint. It is a ball and socket joint with great stability and potentially great mobility. One of the most critical and essential planes of motion and stability is the frontal plane of hip joint motion. This plane (coronal/frontal) of motion and stability is largely determined by the hip abductor muscle (HAM) group through an axis of oriented in the anterior-posterior direction through the head of the femur. The most obvious and simple function of the hip abductor muscles is to produce a movement or moment of abduction of the femur in the acetabulum in the frontal/coronal plane (as in a side lying leg lift). As mentioned, this is a simple way to determine open kinetic chain range and open chain strength in this range but it is neither true nor transferable in theory or practicality when the foot is on the group. When the foot engages the ground the typically usable functional range is much less and the muscular function is now to move the pelvis on the stable and somewhat static femoral head in the frontal plane. Explained in another way, in this closed chain, the insertion of many muscles remains static and the force generated through the muscle will pull at the origin and generate movement at the joint in this manner. In a nutshell, the hip abductor muscles (HAM) will produce either leg motion to the side (abduction) or it will produce a lateral bending or lateral flexing of the pelvis-torso into the same range of motion (abduction).
The most critical and commonly considered hip abductor muscles (HAM) are the gluteus medius, gluteus minimus and tensor fascia lata-iliotibial band complex. These muscles have the most favorable line of pull and all have a femur and pelvis attachment. We will call these muscles collectively the HAM group. In the stance phase of gait the body’s center of gravity (COG) is medial to the hip joint axis of motion. Thus, in this single leg support phase of gait the tendency will be for the body mass above the hip to rotate or drop towards the swing leg side. This gravitational movement should be offset by the concentric, isometric and eccentric muscular activation of the HAM group through the anterior-posterior oriented axis through the head of the femur. Any functional strength deficits (concentric, isometric or eccentric) of the HAM group and/or neighboring synergistic stabilizers will result in an altered joint stability challenge because not only do the HAM and surrounding muscles product movement but they also generated joint compression and thus stability. The possible undesirable outcome may be an altered movement patterning characterized by inappropriate muscle or muscle group activation in either timing, force, speed or coordination with typically coupled muscles. These challenges to the joint and its normally expected movement patterns will result in the body’s search for more stable positions in the frontal, sagittal or oblique planes. These newly established, yet less efficient, positions and patterns of movement are initially welcomed compensations but in time as the new accommodations become rooted in pattern the synergists and other recruitments become overburdened and further demand compensations from other neighboring muscles eventually resulting in pain, joint derangement and dysfunction. These compensations in recruitment and movement eventually will lead to non-contractile soft tissue changes such as hip capsule pattern changes in tension and length. These non-contractile soft tissue changes can not only dictate or perpetuate the newly established aberrant joint movements but help engrain the abnormal movement patterns and their new neurologic patterns.
The Almighty Foot Tripod
You have heard us talk time and time again about the importance of the foot tripod. To review, it consists of the center of the calcaneus, the base of the 1st metatarsal and the base of the 5th metatarsal. To see some of our other posts on the foot tripod, including other exercises, click here
Join Dr Ivo in this brief and informative video demonstrating an exercise that most people with an inadequate foot tripod will benefit from.
Remember Skill, Endurance and Strength. There are many nuances to this simple exercise, don’t take it lightly!
The Gait Guys: Hammering it out, daily, to give you the goods!

Get Certified!
“In my experience, the Foot Wear Certification Series, is what is most needed by anyone in the position of helping an individual receive a more satisfying shoe fit experience. Whether that is a simpler issue of finding the best athletic shoe to enhance their individual health goals, or to assess ones foot anatomy and the problem areas that can be hindering an individuals comfort and ability to function, the videos are informative and deeply educational. The combined experience and knowledge of Drs. Ivo and Shawn Allen is so extensive, that it is the tool I would recommend for those of us in the industry.”![]()
Our 1st IFGEC (International Foot & Gait Education Council) Certified Sales Associate. Congratulations to Julie Meyers; the nations 1st to be certified. Julie works for Dr Waerlop at Summit Chiropractic & Rehabilitation, PC in Dillon, Colorado. She is especially fond of Lemming shoes!
When asked about the exam, she said “Wow, it was really hard!”
Want to get certified? Stay tuned as the program is ramping up!
The Gait Guys. Making gait and foot competency viral!

Hey Guys
Check out these groovy shoes! We wonder if they are carnivorous!
Have a great weekend
Ivo and Shawn
A few months ago we tried something new. We tested your gait auditory skills while listening to a video of a runner on a treadmill. We queued you to listen to the foot falls listening for the one foot to slap or impact harder than the other at foot strike. Most of you got it right, we got plenty of positive feedback on that piece. Here is that piece (link).
This is something we do during the initial evaluation for each and every patient that comes to see us, no matter what their issue. We ask them to walk. We ask them do they notice anything. The answer is almost always, “no”. This is because they are accustomed to their walking habit. The first queue we notice much of the time is that there is either a bilateral heavy heel strike (because heel strike is normal in walking) or it is heavier on one side. We ask them to hear and feel that heavier strike once we point it out to them. Not only can they feel it, they can hear it. It is something they have rarely been aware of until that moment. We then do the same for forefoot loading. If the anterior compartment is a little weaker on one side or if they departed abruptly off the opposite leg for some reason (decreased hip extension, tight calf, loss of ankle rocker etc), a heavier forefoot loading response will be felt and heard as well (opposite side of the mentioned issues). These are great initial gait queues that anyone can use to gain diagnostic information. It also draws the client into greater body awareness of their habitual patterns of movement. We then draw out the numbers and forces for them so they understand what several thousand cycles of this event can cause into their body and their clinical problems they are presenting with. This is typically a new skill they will develop and always be aware of and be able to report to you as they progress through their care with you. Sound and feeling are key biofeedback tools.
Just remember, they are feeling and hearing what they are doing, not what is wrong ! It is your job to take this information and figure out the “Why” it is happening, and the “how” to fix it. This is the hard part.
Hey Folks
You know we are big Altra Fans. Check out their new commercial!
We are sure your keen eyes have picked up on the midfoot pronation at :17 and forefoot pronation at :28. This brings to mind a question we often get asked: How much pronation is too much pronation?
Some pronation is necessary, as it is one of the 4 shock normal absorbing mechanisms
We do not believe there is a perfect answer, but rather the ideal is: How much pronation can your (neuro and bio) mechanics control? Too much in one individual may be not enough in another. It has to do with foot structure, muscle competency, neuromuscular control, and a host of other things.
Remember the mantra: Skill, endurance, strength… in that order! Work to control the pronation you have and expand on that range.
The Bald Headed, Good Looking, Bringing you the facts Gait Guys.
all material copyright 2012 The Homunculus Group/The Gait Guys (except the commercial of course, which is property of Altra). If you want to use our stuff, ask nicely : )

Got Hip Pain ? Attention Runners and Athletes with Hip Pain.
Compensatory joint motions are quite often a source of a person’s pain. Shirley Sahrmann named her hip syndromes for the direction of the movement most consistently associated with pain. In a recent CME presentation we did for www.onlineCE.com we discussed the accessory movements found with the hip.
Lets look at the known normal biomechanical facts:
During hip flexion the accessory motion is posterior glide of the femoral head.
Hip extension: accessory motion is anterior glide of the femoral head.
Hip medial (internal) rotation: accessory motion is posterior glide of the femoral head.
Hip lateral (external) rotation: accessory motion is anterior glide of the femoral head.
Hip abduction: accessory motion is inferior glide of the femoral head.
Hip adduction: accessory motion is superior glide.
Impairment, either from joint/bony deformation (ie. torsions) or from functional muscular asymmetry, can lead to impairment of the accessory motions (compensation) that are necessary for clean joint function. This can lead to pain.
For you clinicians out there, knowing your hip torsions and versions will impact the amount/degree of these accessory motions. This is why we harp on knowing your fixed anatomic variants. (You can find discussions on these in our prior blog posts and on previous recorded www.onlineCE.com teleseminar presentations.) For example, reduced medial rotation at the hip (usually met with increased external rotation) is often seen in people with retrotorsion of the femur. Said another way, when your client has impaired medial or lateral hip rotation you must go beyond looking at the muscles at some point and consider whether they have a form of ante or retro torsion.
Hip extension is a critical part of normal human ambulation, whether you are walking or running. Normally the hip, when moving into extension during the final propulsive phase of ambulation, allows for the femoral head of the hip to glide anterior in the socket (acetabulum). This reduces labral RIM pinch (RIM Syndromes) and allows for greater safe extension range. If hip extension range is impaired then this accessory motion of anterior glide can be impaired and lead to compensation and pain.
Think about this:
What if the quadriceps are tight ?
What If the Glutes are weak ?
What if rotational muscles are short ?
What if ankle rocker (dorsiflexion) is impaired ?
What if there is neuro-inhibition from joint pain (ie. osteoarthritis or joint mal-centration etc) ?
What if there is imbalance and weaknesses about the hip ?
What if there are other faulty movement patterns ?
What if there is one of the femoral torsions present ?
Much of this is “chicken or the egg”, who came first ? These “what ifs” are what make practicing medicine difficult and a real challenge. Some of these issues can be found during functional movement assessments, but some of them will be missed if that is all you are doing. These issues may be what separates the good clinician, therapist, coach or trainer from the “not so good”. Knowing if a person has an impaired rolling pattern (see here http://youtu.be/dqnR0EcW2YY) is great to know, but knowing if the lower limb driver is off because the hip cannot internally rotate is even greater. Merely giving the person the homework of practicing and repeating the rolls on the impaired driver side without assessing all of the parts (for example some of the issues above) may cause you to miss the boat, or to engrain a new faulty motor pattern.
Knowledge is prince, application of knowledge is king.
Next week we will begin a blog post a week on the biomechanics of the hip. We hope you will join us.
Shawn and Ivo
Here are some of our prior blog posts to add and deepen this dialogue:

Donate here











Help keep us free ! Make a donation by clicking. here.

Donate to get exclusive content from The Gait Guys
OUR SEARCH BOX IS INTUITIVE, TYPE IN YOUR KEY WORD, WAIT, THEN SCROLL DOWN.
Email us: our email is found under the "Disclaimer" Tab above.

Powered by Squarespace.