

Hip Biomechanics: Frontal Plane Part 3
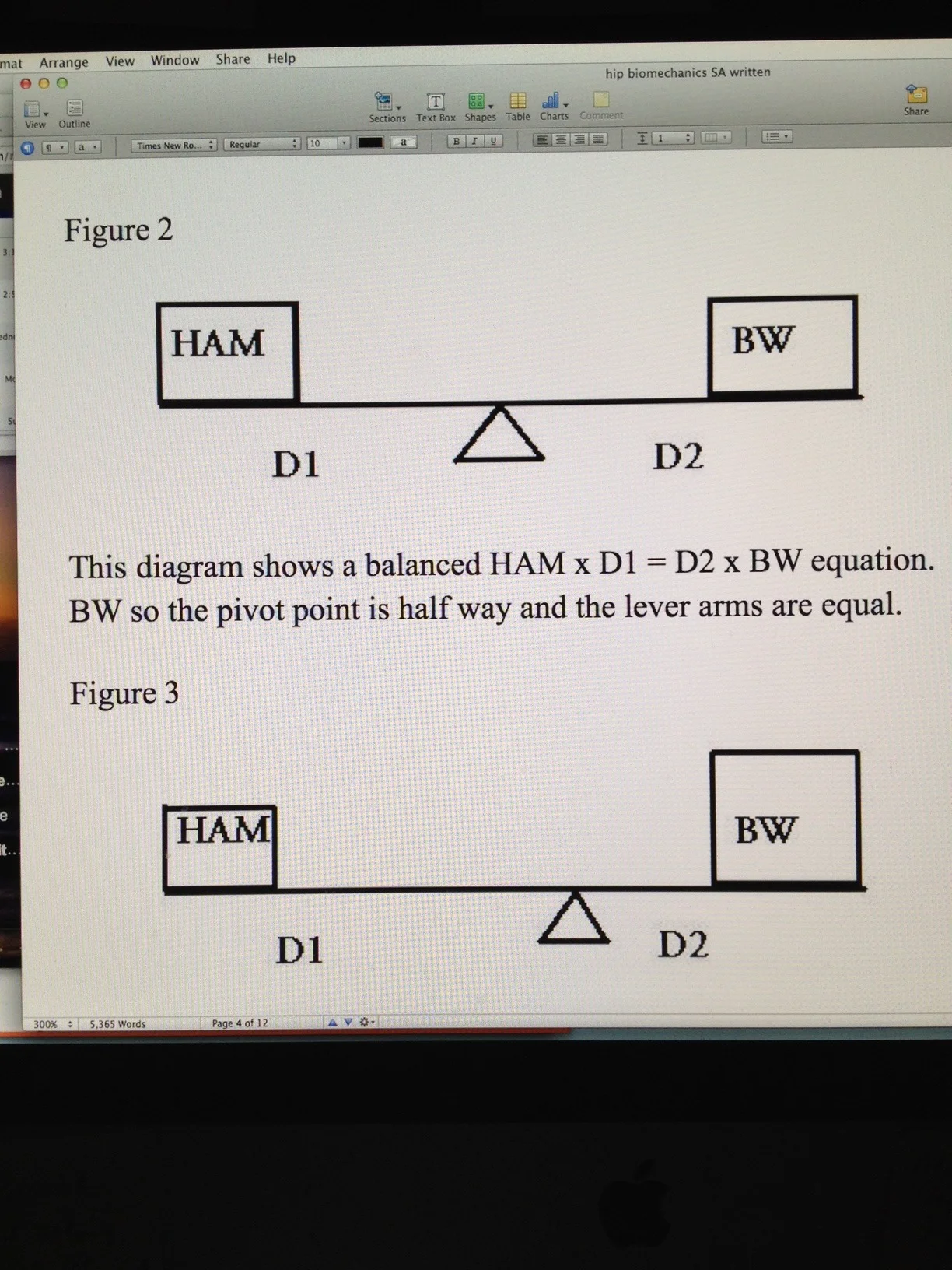
This diagram (Figure 3) also shows a balanced HAM x D1 = D2 x BW equation. The BW is larger than the HAM but this is offset in the rules of the teeter-totter. Shifting the pivot point towards the larger mass is offset by the smaller D2 and larger D1 moment arms. This is a typical compensatory mechanism used by obese patients to ambulate effectively. It does render significant frontal plane movement of the pelvis instead of the more desirable silent frontal plane pelvis. In this compensation, even large body weights can be somewhat offset by the degree of contralateral hip hiking to reduce the D2 moment arm and increase the D1 moment arm however this compensation has its limits. When the limits of alteration of moment arm length are reached the body’s only compensation at that point is to increase the HAM forces which increases joint compression and thus cartilage wear since the cyclical loading and unloading of the cartilage is much less. This is also the same mechanism used by patients with a osteoarthritic painful hip joint. We are not referring to increasing BW, rather we are suggesting that to reduce pain the patient will want less joint compression and thus a reduced HAM. To do this we want to increase the D1 moment arm. The only way other than surgery to achieve this increase in D1 is to take the existing body weight and shift it closer to the pivot point. Ideally you would want to lean so far over the affected painful hip as to get your body weight (BW) immediately over the pivot point. This is what is done with a walking cane in the opposite hand of the stance leg, to help lift the swing phase leg and pelvis and to push the body mass over the hip WITHOUT using more HAM (glute medius contraction generated compression, which would generate pain). This would effectively reduce D2 to nil and significantly increase D1 thus allowing HAM to be minimal; thus reducing painful joint compression. (In teeter-totter verbiage, put the small child on the long part of the teeter-totter arm and you can move large forces with little effort at the pivot point.)





























