Much like the excessive wear on this left heel (see photo) it merely tells you that the person is, FOR SOME REASON, impacting/scuffing that heel too much. It too does not tell you why they are moving that way. (The shoe case explained in a moment).
Giving someone a "corrective homework exercise or stretch" or new movement because you "think" they are failing a screening procedure is nothing more than confirmation bias on your existing knowledge base (which for ALL of us is limited, yet hopefully expanding). Your confirmation bias might be, "I know what this screen should look like, I know what my gurus have told me it should tell me, and this client just failed the screen, so here is what you need to do to make the screen look and test better and here is what will make the client "better" (whatever that is)."
It just cannot, and is not, that simple.
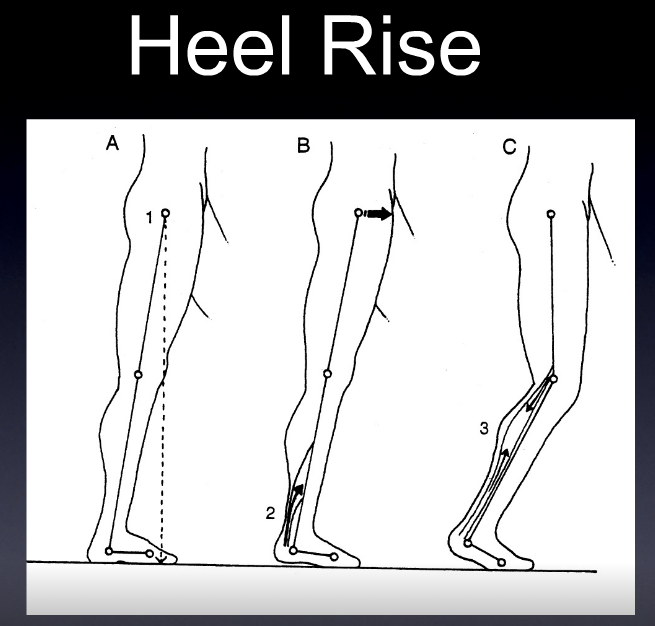
Similarly, it would be like telling this person not to heel strike so hard, "Stop heel striking, stop scuffing your heel !". It is just not that simple and it is foolish to think so. We need to get to the bottom of the problem, the root cause. This means we need to hands-on examine our client, and correlate said findings to the screens. Collectively, we are just gathering information to put together a cause effect for any of our patient's problems. But you cannot just make assumptions that stroke your confirmation bias. There is logical process in place, for a good reason.
Now, why is this guy scuffing his left heel? He has no left heel pain, no left leg pain, clean foot, ankle and hip mechanics on that left side (from detailed coupled screens correlated with a detailed hands on exam including neuromuscular strength, length, skill, length-tension relationships, endurance assessments etc).
And if you think we are not guilty or above all of these mistakes we are calling out, you are mistaken. WE are on the same bus as everyone else. WE are human, we have biases, so we have to check them everyday. Just the other day I told a patient he wasn't getting better because i made and assumption based off of what i saw in his gait, and i assumed he wasn't going to fail my hop test, that it was a different problem, so i looked elsewhere, found something that confirmed my bias, and they came back 2 weeks later saying "i did my homework, i am no better." I took them into the hallway, had them go through my hop screen, and damn if i wasn't ashamed of myself, i followed with some hands on exam, and dang if I wasn't a confirmed moron. So, we screw up too, more than we like to. Some people will say "that is why we call it a medical practice". That is a soft let down. Sure, it happens, but laziness and confirmation bias happens way more often in all of us we believe.
Look at the cartoon below, the parents think the kid loves the animal mobile. From their perspective, from their limited experience lying under an animal mobile, how could they know the kid was smiling because he/she was looking up at 4 anuses? Four puckered anuses (yes, the plural is not ani. We had to look it up, too !). Go ahead, laugh, we did.
*And so, if you do make corrective exercise recommendations off of a screen, without clinical hands-on exam correlation, may your kids paint animal anuses on your bedroom ceiling to remind you of their tortured infant years.
Perspective, like this infant here staring at buttholes of stuffed animals, is amazing. It is all too often how you approach things, and with the limited (or expansive) knowledge and experience you approach it with, as to what confirmation biases you lay on things, and how you go about solving things.
*Oh, as promised, this dude in the shoes, has markedly weak RIGHT hip abductors and RIGHT lateral core (from our hands on exam and then specific loaded screens to assess and help confirm these things). This means, right lateral pelvis drift. This confirmed the visual drop of the left hemipelvis during swing phase, which allowed the left foot to have challenged clearance (he could hear the heel scuff when walking). Yes, slight left cross over gait too. The corrective exercise is to improve the right hip and lateral core stability, and establish gait awareness homework to learn how to reengage those areas. The corrective exercises were not to force more LEFT hip flexion and knee flexion to gain more clearance and stop the heel scuff. A monkey could figure that out. But that would seem logical if no examination had been done.
PS: There is no need to check his pelvic floor (see infant mobile cartoon above to extrapolate that joke). But, if you made assumptions of what homework to give him based only off of a bunch of screens, heck, you might as well check his sphincter. What do you have to lose?
WE would LOVE, love love love to give credit to whoever drew this cartoon. There is no name on it, we NEED to give them credit. It is more than brilliant. IT is an entire lecture on perspective. Send us this genius person's contact if you know who it was ! Please !!!!!!
Shawn Allen, the other gait guy
#gait, #gaitproblems, #gaitanalysis, #movementscreens, #correctiveexercises, #thegaitguys, #heelstrike