A Case for “Reverse Engineering”
You have often heard us say: “think of muscle function from a closed kinetic chain perspective”. In other words, the muscle(in the case of gait) working from the foot (or ground) up. Here is a study exemplifying this with the tibialis anterior and peroneus longus.
We remember the tibialis anterior is usually the most prominent muscle on the anterior leg (see 1st 2 pictures above). It has two origins, the lateral tibial condyle and the upper lateral surface of the tibia; it inserts on the medial surface of the 1st (medial) cuneiform and proximal part of base of the first metatarsal of the foot. It is a dorsiflexor and inverter of the foot in open chain (ie before and at heel strike/initial contact), and a dorsi flexor and inverter of the foot (or it brings the tibia medially and everts the foot relative to the tibia) from loading response to midstance. It also helps to maintain the medial longitudinal arch up to this point, and assist in decelerating pronation (along with its antagonist to dorsiflexion, the tibialis posterior). It takes a break at midstance and then contracts again at terminal stance (to counter act its antagonist, the peroneus longus). When running, it remains active through midstance to help pull the leg forward over the foot.
The authors have this to say: “Tibialis anterior restrained rearfoot plantarflexion from heel contact to 10% stance, and eversion between 10% stance and footflat.”
No surprises here.
Now the peroneus longus: “Activity in peroneus longus was consistent with its role in causing eversion after heel contact, then as a stabiliser of the forefoot after heel rise. ”
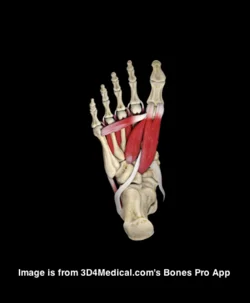
The peroneus (or fibularis) longus arises from the head and upper two-thirds of the lateral surface of the fibula, from the deep surface of the fascia, and from the intermuscular septa between it and the muscles on the front and back of the leg; occasionally also by a few fibers from the lateral condyle of the tibia. You can see from it attachments that it can influence the entire upper lateral leg.
It’s tendon runs down the fibular shaft, wraps around the lateral malleolus, travels obliquely under the foot, crossing the lateral cubiod (which it everts after midstance to help with supination) crosses the sole of the foot obliquely, and inserts into the lateral side of the base of the first metatarsal and lateral aspect of the 1st cunieform.
It acts from just prior to heel strike to limit excessive rearfoot inversion, through midstance to decelerate subtalar pronation and assists in stabilization of the midfoot articulations, and into terminal stance and pre swing to lock the lateral column of the foot for toe off and plantar flex the 1st ray (creating a good foot tripod), allowing dorsal posterior shift of the 1st metatarsal-phalangeal joint axis (necessary for dorsiflexion of the hallux (big toe)).
The peroneus brevis arises from the lower two-thirds of the lateral surface of the shaft of the fibua and from the intermuscular septa separating it from the adjacent muscles on the front and back of the leg. Again. lots of influence here.
It travels behind the lateral malleolus (and in front of the peroneus longus) and inserts into the tuberosity at the base of the fifth metatarsal.
It acts in a similar timeframe as the longus, copressing the tarsals to provide midfoot stabilization, and a significant eversion moment of the foot (helping to push you on to the base of the 1st metatarsal).
You can see how the peroneii could work together also to produce a small plantar flexion moment of the ankle and lateral movement of the lower leg. Because of their route around the lateral malleolus, they also can internally rotate the tibia (from a closed chain perspective; remember the tibia SHOULD be extenally rotation at this this point) so it can act to dampen or attenuate supination. This is also supported by the study:
“Activity in peroneus brevis suggested a role in restraining lateral rotation of the leg over the foot, late in stance.”
We are definitely the Uber Gait Nerds of the internet. We are bending your mind around the foot (rather than the foot around your mind).
Ivo and Shawn
Abstract
This study examined stance phase foot kinematics, kinetics and electromyographic (EMG) activity of extrinsic muscles of 18 healthy males. Three-dimensional kinematic and kinetic data were obtained via video analysis of surface markers and a force plate. Ankle joint moments are described about orthogonal axes in a segmental coordinate system. Kinematic data comprise rearfoot and forefoot motion, described about axes of a joint coordinate system, and medial longitudinal arch height. Surface EMG was obtained for tibialis anterior, soleus, gastocnemius medialis and lateralis, peroneus longus and peroneus brevis and extensor digitorum longus. It was concluded that the demands on the controlling muscles are greatest prior to foot flat and after heel rise. Tibialis anterior restrained rearfoot plantarflexion from heel contact to 10% stance, and eversion between 10% stance and footflat. Activity in peroneus longus was consistent with its role in causing eversion after heel contact, then as a stabiliser of the forefoot after heel rise. Activity in peroneus brevis suggested a role in restraining lateral rotation of the leg over the foot, late in stance.
Extrinsic muscle activity, foot motion and ankle joint moments during the stance phase of walking.
School of Physiotherapy, Faculty of Health Sciences, Lidcombe, NSW, Australia. a.hunt@cchs.usyd.edu.au
Erratum in
- Foot Ankle Int 2001 Jul;22(7):543.