The London Looter’s Getaway Stride: Gait analysis by The Gait Guys
We did this one yesterday in collaboration with our good friends at Zero-drop.com on their awesome blog. Check out their stuff.
The images coming out of England of young hoodie-wearing hoodlums rioting, stealing, smashing store windows, torching cars, and causing all-out mayhem in London and elsewhere is unsettling for several reasons. What exactly are these lawless yobs protesting? Are these race-induced riots? Public outcry over political and social injustice? Or are these roaming gangs of hooligans more interested in something else–like getting their hands on free stuff such as 46-inch flat-screen high-definition televisions and Nike sneakers.
In the photo here, it appears as though a young lad has just swiped a bottle of something lip smacking from a Manchester food store. It seems that he dressed for the occasion –Adidas track suit and running shoes– to facilitate a quick, speed getaway. He’s much too young to be hitting the bottle. Plus, one can easily assume that he didn’t expect to make the front page of the U.K. Daily Mail where this photo first appeared. (He’s probably sitting right now in juvie detention.) In any case, Zero Drop asked the Gait Guys to look at his running stride. Here’s their expert analysis:
__________________________________________________________________________
This chap looks a bit young to be drinking, and we doubt he is a courier. Let’s see if he will make a clean getaway, shall we?
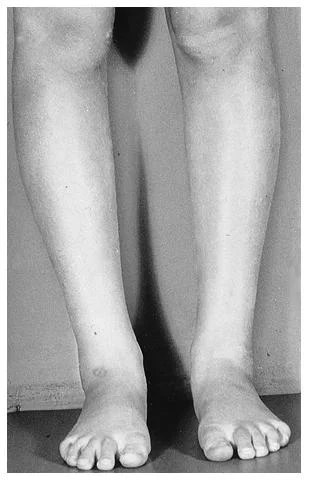
Beginning from the bottom, we see his left foot is turned in and his knee appears straight, He does appear to be banking a left turn, but we would expect him to probably have his toe out a bit for stability since he is really banking heavily into the frontal plane (he must have a great right gluteus medius because he is holding a fairly decent pelvic line into the bank), so our guess is he has a bit of internal tibial torsion (i.e., his foot points in when his knee is straight ahead. This is usually a condition from birth). Folks with internal tibial torsion tend to have their feet in supination more, so they are excellent levers, but it usually means they lack some shock absorption (so maybe we find a forefoot valgus in that shoe, who knows). Because his knee is not in line with his line of forward progression, there will be a conflict there, which could potentially hurt his knee, besides cutting down on his mechanical efficiency (the knee is like a door hinge, and works best when moving in one direction).
His lean to the left nicely complements his probable forefoot varus (or inversion of the forefoot), so at least he has that working for him. There is a little hip sag on the left, indicating a weak gluteus medius on the right; which further cuts down his mechanical efficiency; it is moving to the right as he is cutting to the left. Holding that bottle sure cuts down on his arm swing, and he looks a bit tense, as his left shoulder is higher than the right. Like he is trying to hide something. Finally, his head posture looks forward. This facilitates his flexors and inhibits his extensors, taking away from power to drive him forward. We could go on and on, and we have. Guess we told you how to build a clock and you only wanted to know what time it is. In short, whether he gets caught depends on the biomechanics of his pursuer.
We hope he doesn’t have internet access to our blog, we would hate for him to recognize his problems and improve upon them. We would be contributing to improved “get-aways” in the future. That wouldn’t be good, unless someone was chasing him with a .22 , then we might feel ok with it.
Hooch for the youngers, it’s not just for the back alley’s anymore !
- the gait guys