Upright bipedal walking and the stoned chimpanzee.
How different is our human gait to the chimpanzee gait ? Months ago we did a blog post on the Sasquatch aka Bigfoot. You can find our blog post here (click). Bipedal walking is evident in the earliest hominins [Zollikofer CPE, Ponce de Leon MS, Lieberman DE, Guy F, Pilbeam D, et al. (2005) Nature 434:755–759], but still today the true reason as to why our unique two-legged gait evolved remains unknown for certain. Scientists 7 years ago found fossil evidence in Ethiopia that showed human ancestors walked on two legs as early as 5.2 million years ago. The fossils were of the earliest hominid known, and dated from close to the time when human ancestors are believed to have split off from the chimpanzees on the first steps of their evolutionary trip to modern Homo sapiens.
Our point here today is just to briefly discuss a few of the biomechanical characteristics of the chimpanzee gait and to correlate them to problems we see in human gait. Our point however is not to bring up issues of evolution, creation or anything of the sort that might offend anyone’s beliefs (however at the end of this piece we do have some creative “outside the box” fun thinking and offer some challenging possibilities in correlating them to theories of how man’s brain might have grown so suddenly and possibly where the advancement of complex motor patterns evolved).
This time we look at the chimpanzee. How does the chimpanzee differ from the gorilla in quadrupedal ambulation ? Both walk with a knuckle-type weight bearing but chimpanzees ambulate quadruped with bend wrists, their carpal bones have ridges and grooves like humans that allow for end range lockout while gorillas quadruped via straight arm and neutral wrist knuckle weight bearing.
But what about humans and these hairy precursors ? Are there similarities ? Differences ? Well, the main question we wanted to ask since apes were not far enough evolutionarily to walk effectively upright is, “are there similarities to pathologic gait problems that lead to injury and these hairy ancestors ?”. We believe the answer is yes.
- posteriorly tilted pelvis
- small weakended glutes
- quadriceps dominant
- lack of knee extension
- lack of hip extension and gluteal development
There are many interesting thoughts here. Including the question that the documentary video above poses in part 2 found on youtube. Can two species with 99% of the same DNA have similar problems? Should they? The numbers are in favor of this theory. It also bodes the question that recurs in the video series on Oliver the chimp, if he is even closer to human DNA than his siblings then is this why he walked upright like us humans ?
article link: http://www.pnas.org/content/104/30/12265.full
In this article link above, the authors support the possible hypothesis that energetics played an important role in the evolution of bipedalism. Unfortunately there still remains an evidence gap archaeologically to fully support this hypothesis that locomotor economy provided the initial evolutionary advantage for hominin bipedalism. The study above indicated that
“the biomechanical analysis of adult chimpanzee costs, coupled with previous analyses of early hominin pelvic and hindlimb morphology, suggest that improved locomotor economy may have accrued very early within the hominin lineage. Future fossil discoveries from the earliest hominins will resolve whether this energetic advantage was in fact the key factor in the evolution of hominin bipedalism.”
Similar to this study, some sources discuss that moving to an upright gait is what caused our brains to suddenly expand in size and thus begin to cerebrally dominate all other creatures on earth. This does however remain a hotly debated topic. Our recent interests on these topics have brought us far and wide. Topics on brain expansion have included the strategizing of carrying infants, food and weapons for distances to hunt for food to being able to run distances more efficiently to hunt. Language (complex communication verbally and with symbols), art (cave wall paintings), religion, spiritual belief development and developing the manual dexterity and complex thinking to build and use tools for specific tasks are just some of the other reasons as to what spurred the massive growth of the human brain roughly 50,000 years ago (Google search “brain expansion 50,000 years ago”).
But, if you really want to challenge your beliefs on the topic of brain size expansion and the development of complex neurologic patterning read some of the fascinating work by Graham Hancock or Terrance McKenna on ayahuasca (yes, The Gait Guys are about to talk about mind expanding hallucinogenic drugs). From Wikipedia,
Ayahuasca (ayawaska pronounced [ajaˈwaska] in the Quechua language) is any of various psychoactive infusions or decoctions prepared from the Banisteriopsis spp. vine, usually mixed with the leaves of dimethyltryptamine (DMT)-containing species of shrubs from the genus Psychotria. The brew, first described academically in the early 1950s by Harvard ethnobotanist Richard Evans Schultes, who found it employed for divinatory and healing purposes by the native peoples of Amazonian Colombia, is known by a number of different names (see below). It has been reported that some effects can be had from consuming the caapi vine alone, but that DMT-containing plants (such as Psychotria) remain inactive when drunk as a brew without a source of monoamine oxidase inhibitor (MAOI) such as B. caapi. “
You may find it interesting that some new age theories by gentlemen such as mentioned above propose that it was the use of these hallucinogenics containing DMT as well as Psilocybin (aka magic mushrooms) as possible mechanisms for the massive growth of the human brain and subsequent abilities to tackle more complex motor tasks, especially those that incorporated ambulation.
Think that we, and these men, are a bit crazy ? That is ok, probably many folks already think that. But heck, even in some sources that discuss what was present in the Garden of Eden show possible evidence of this wild theorizing because according to several sources the "potential forbidden fruits of the Garden of Eden include the apple, pomegranate,the fig, the carob, the etrog or citron, the pear, and, more recently, the datura (a hallucinogenic) ( were all present). And, "A fresco in the 13th-century Plaincourault Abbey in France depicts Adam and Eve in the Garden of Eden, flanking a Tree of Knowledge that has the appearance of a gigantic Amanita muscaria, a poisonous and psychoactive mushroom”, was also possibly present. Now, do not put words in our mouths, we are not saying by any stretch of the imagination that Adam and Eve were stoners. McKenna and Hancock and many others merely theorize (with logical inquiry) that at some point in history, they believe around 50,000 years ago, that mind expanding drugs may have helped force the brain to develop by experiencing cerebral alternative phenomena that the real world was not able to offer. And it is postulated that this brain expansion is what has allowed higher function and higher cognition. And if you think we are crazy to even bring this up as a possibility you might consider doing your own investigations looking into the minds of some brilliant and educated people in science today. You will find that some of them will not dismiss this seemingly radical topic as the reason for the massive and sudden expansion in brain size. Yes, like some of these researchers we are pushing the limits here, but who are we to say that we know the truth any better ? None the less, this blog is not the place to discuss mind expanding hallucinogenics, although we are happy to offer it as just one of the theories of wiser men and women to wet your curiosity to wilder ideas ! Heck, something made our brains suddenly expand some 50,000 years ago. We had millions of years for it to happen, so why was it right around 50,000 years ago ? Because that was the first documented evidence of mind altering natural (yes, organic) herbals? Professor Davis Lewis Williams apparently thinks so. It certainly would have been easier to reach down and grab some leaves and vines or mushrooms wouldn’t it ? Take today’s post with a grin, a pinch of salt, and a pinch of curiosity !
And to further tease your mind to open up, do you wanna guess who else might have done a little substance experimenting ? Search the web for “Einstein and drugs”. One source claims that Einstien’s blood was tested after his death with the autopsy apparently showing traces of LSD as well as Dimethyl-triptimene (DMT). Still wondering how he got so smart ? Hmmm. Now, if you do your homework you will find that DMT is a natural chemical in the body as well as in many plant types, it is a chemical possibly involved with the pineal gland. Many theorize that the dream state we experience every night is from the natural low levels of DMT in our brain, it is possibly why our dreams are so wild and wonderful. But DMT is found in many foods as well, we just break it down with MAO (mono amine oxidase). This is why the psychadelic trips with DMT require a MAO inhibitor to the drug can do its thing. Anyhow, enough drug and brain education for today………
Einstein and many others…….. smart, big brained, world changing folks, many dabbling in mind expanding substances. Heck, how else does one come up with String Theory, Dark Matter, Black holes, Space-Time continuum etc ? Maybe you have to be thinking outside the box and possibly tapping into another dimension to come up with such broad thoughts. Who knows ? Kinda makes you wonder what you might have missed out on in college doesn’t it … if in fact you missed out on it.
The “Stoned Ape Theory” tangent. It is a very radical extreme theory for brain size expansion 50,000 years ago. But radical theories are cool, they make you stretch your thinking and comfort zone. And they just might be true , who knows ? If we can for a moment put aside preconceived biases, old education and embedded religious beliefs and open our mind and thinking we just might see things that expand our wisdom. That’s the hard work. It doesn’t mean we have to accept them. Challenging radical ideas can do that if you can open your curiosity. Regardless, paleo brain or neo brain , we ambulated with both. Brain expansion changed gait, because it changed what we do while we ambulate. And then we changed it all further by adding shoes and paving the surfaces of our world.
Shawn and Ivo…… more than just gait geeks but certainly not Stoned Apes. Maybe just two guys here to further expand the brains of 21st century man with theories on gait and biomechanics.



































Here is a long Q and A Dr. Ivo had with a client who emailed us quite awhile back. It is very informative and it has links to the readers gait videos. We hope you find this informative.
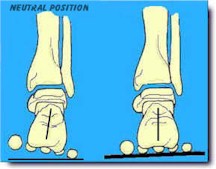
Q: I am a long time distance runner (33 years of marathoning so far ) that has had back and hip problems since the 1980’s. I have tried all sorts of therapies, but I have a funky stride on my left side. I started going to an ART doctor this week. He said I have an inverted heel on the left side and functional hallux limitus on both sides, however on the left side (with the inverted heel) the foot pronates down to get the first metatarsal to touch the ground. So my left heel supinates and the forefoot pronates and does this strange movement that creates havoc with my leg and hip (at least that is my understanding).
By checking out your videos, is rearfoot varus the same as inverted heel? or is there something else you can point me to. I am getting ART treatment for the heel, mobilizations on the foot, and the doctor suggested cutting out part of a Dr. Schools ¾ foot insole underneath the first metatarsal to see if this makes the toe and metatarsal work.
You can see short videos of my funky left foot stride here: http://recoveryourstride.blogspot.com/2010/06/inverted-heel.html
Any thoughts or advice would be much appreciated.
Jim