

We have been trying to classify some of these gaits and are looking for a government grant to do so….. We figure they may have a short leg or two….
The Gait Guys at the Movies: Terminator 2→
/The Gait Guys at the Movies: Terminator 2. Here is a spot we did for Natural Running Centers………fun stuff, good data. We hope to offer a more technical version soon, with more details but for now……..Enjoy
Is it possible to take 3 minutes off your half marathon ?
/An article by Michael Warburton, published as an Internet post on barefoot theory, seemed to spark some of the resurgence of the method of running. In his brilliant 2001 piece he had some interesting thoughts and pointed out some noteworthy facts. He indicated that research showed that an extra mass of 100 grams attached to the foot diminished the economy of running by one percent. Thus, two 10-ounce shoes (the weight of a lightweight training shoe) could have a compounding crippling effect on efficiency by more than five percent. In tangible terms, that could be more than six additional minutes for a world-class marathoner, taking a world record to a mere first-group finish.
link to Warburton article: http://www.sportsci.org/jour/0103/mw.htm


Pronation Primer: Part 2
The problem with OVERPRONATION
The consequence of under or over pronation ultimately means other articulations, including the spine, will have to attenuate more shock. Over time, this may lead to articular cartilage degeneration, disc degeneration, or ligamentous laxity, due to repetitive stresses.
What about assymetrical pronation?
It is rare that people over or under pronate the same amount on each side. Excess midfoot pronation on the right causes more internal rotation at the right knee (see above picture), and an increased valgus stress here. This puts the quadriceps at a mechanical disadvantage and stretches the adductor group, often making them stretch weak, and shortens the abductors, especially the gluteus medius, which often becomes short weak. The right foot, since it is now a poor lever, will often be externally rotated and toes claw, because the center of gravity has moved medially and they are trying to make that limb stable to bear weight on so they can progress forward. They will often toe off from the inside of the great toe (as is often evidenced by a pinch callus here). The medial rotation of the lower leg causes internal rotation of the thigh and anterior nutation of the pelvis on that side, both which now put the gluteus maximus at a mechanical disadvantage, limiting hip extension on that side. Now the extension has to occur to somewhere, so it often occurs in the lumbar spine, along with rotation and lateral bending to that side, increasing compression on the right facets. Now the vestibular system kicks in to right the head and we get contraction of the left paraspinals. Arm swing usually increases on the contralateral side to assist in propulsion forward. What effect do you think THAT has for about 10 thousand steps a day on spinal mechanics? What effect are we having on the nervous system and what neuroplastic changes are occurring? Hmmmm….
Having both feet planted on solid ground, or rather having both feet planted solidly on the ground should concern you. As you can see, knowing about pronation and its effects on the entire kinetic chain is paramount to the clinician. The effects reach far beyond the foot and can often be the root of recurrent biomechanical faults in the human frame.
And some people thought it was as easy as slipping an orthotic in there…
Yup, we still are….The Gait Guys
Advanced Gait and Running Topics: Biomechanics, Details of Foot types, Multiple Case Studies→
/another course offering is now available for your viewing.
The course by The Gait Guys, Biomechanics 203: Advanced Gait and Running Topics: Biomechanics, Details of Foot types, Multiple Case Studies. 3 hour lecture, segemented. This is one of our long awaited courses. Tons of detailed materials in this course. (available for 3 hours continuing education).
Whether you are looking for continuing education credits, or just looking to learn more about true foot function and how it integrates with the rest of the body…….this is a great lecture.
- More discussion on the walking and running gait cycles
- Apply the biomechanics of the pelvis and lower kinetic chain during walking to clinical practice
- Predict and discuss problems and clinical strategies that can arise from altered lower extremity biomechanics
- Apply visual analysis skills
- Evaluate case studies in gait analysis
- Clinically apply solutions for gait abnormalities
- video case studies mingled into each topic
Click the link above, when you get to the website, choose CONTINUING EDUCATION COURSES, and from the pull down menu select CHIROPRACTIC DOCTOR. Look under BIOMECHANCS, select course 203.
Enjoy


Pronation Primer: Part 1
A lot of folks seem to be on a mission to eliminate pronation, calling it the scourge of humanity and source of human ailment. While we agree that overpronation causes biomechanical faults in the lower kinetic chain, so does under pronation, and some pronation is necessary and required for normal locomotion. We hope this post serves to clarify any misconceptions there may be about it.
When most people think of pronation, they think of midfoot pronation, or pronation about the subtalar or transverse tarsal joints. Pronation can actually occur about any articulation or bone, but with respect to the foot, we like to think of rearfoot (ie. talo-calcaneal), midfoot (talo-navicular) and forefoot (transverse tarsal). The question is why does this matter?
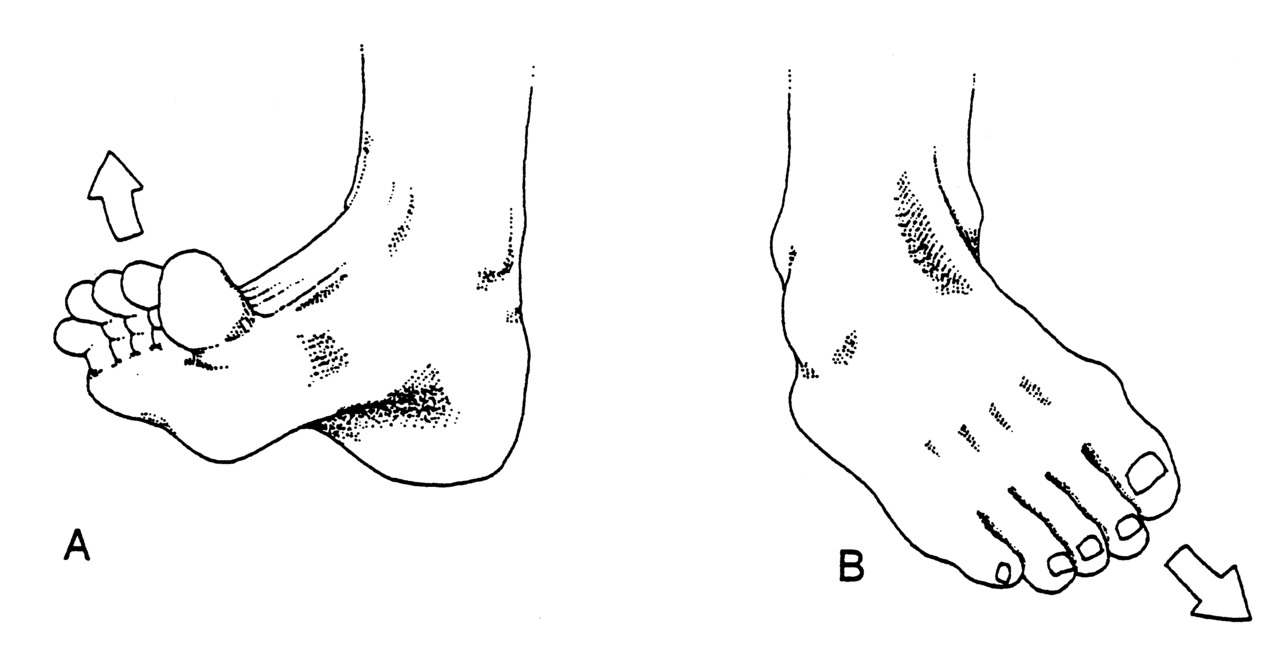
Pronation, with respect to the foot, is defined as a combination of eversion, abduction and dorsiflexion (see picture attached) which results in flattening of the planter vault encompassing the medial and lateral longitudinal arches. In a normal gait cycle, this begins at initial contact (heel strike) and terminates at midstance, lasting no more than 25% of the gait cycle.
In a perfect biomechanical world, shortly following initial contact with the ground, the calcaneus should evert 4-8 degrees, largely because the body of the calcaneus is lateral to the longitudinal axis of the tibia. This results in plantar flexion, adduction and eversion of the talus on the calcaneus, as it slides anteriorly. At this point, there should be dorsiflexion of the transverse tarsal (calcaneo-cuboid and talo-navicular joints). Due to the tight fit of the ankle mortise and its unique shape, the tibial rotates internally (medially). This translates up the kinetic chain and causes internal rotation of the femur, which causes subsequent nutation of the pelvis and extension of the lumbar spine. (Hmm, this is beginning to sound like a common cause of low back pain) This should occur in the lower kinetic chain through the 1st half of stance phase. The sequence should reverse after the midpoint of midstance, causing supination and creating a rigid lever for forward propulsion.
Pronation, along with knee and hip flexion, allow for shock absorption during throughout the 1st half of stance phase. Pronation allows for the calcaneo-cuboid and talo-navicular joint axes to be parallel making the foot into a mobile adaptor so it can contour to irregular surfaces, like our hunter gatherer forefathers used to walk on before we paved the planet. Problems arise when the foot either under pronates (7 degrees valgus results in internal tibial rotation), resulting in poor shock absorption or over pronates (> 8 degrees or remains in pronation for greater than 50% of stance phase).
Wow, kind of overwhelming, eh? Stay tuned for part 2 tomorrow.
We remain….The Gait Guys…Telling it like it is…..
The Gait Guys, Biomechanics 202: Foot Function and the Effects on the Core and Body Dynamics→
/Now available for your viewing.
The course by The Gait Guys, Biomechanics 202: Foot Function and the Effects on the Core and Body Dynamics
Whether you are looking for continuing education credits, or just looking to learn more about true foot function and how it integrates with the rest of the body…….this is a great little lecture.
- Describe how the motor and sensory homunculus relate to the foot and are integral to training and rehabilitation
- Discuss the 3 rockers of the foot
- Give examples of problems that result from a loss of the 3 rockers of the foot
- Explain the concept of pelvis neutrality and its effect on training
- Describe and examine the tripod of the foot
- Breakdown most movement into 2 basic rules or tenets
- Give examples of the problems which can arise if the 2 basic rules or tenets of movement are not followed
- Discuss the clinical consequences of loss of the medial and lateral tripods of the foot
Click the link above, when you get to the website, choose CONTINUING EDUCATION COURSES, and from the pull down menu select CHIROPRACTIC DOCTOR. Look under BIOMECHANCS, select course 204.
Enjoy
The Gait Guys: Proper Shoe Selection and Foot Types.→
/Now available for your viewing.
The course by The Gait Guys, Biomechanics 204:
- Describe and identify how the parts of a running shoe affect running biomechanics
- Compare and contrast different shoe constructions to the biomechanical needs of an individual
- Determine the appropriate last shape for different foot types
- Discuss the biomechanical consequences of improper vs. proper selection of last types
- Predict which features in a shoe are necessary to correct faulty gait patterns
Whether you are looking for continuing education credits, or just looking to learn more about shoes and proper shoe type, etc…….this is a great little lecture.
Click the link above, when you get to the website, choose CONTINUING EDUCATION COURSES, and from the pull down menu select CHIROPRACTIC DOCTOR. Look under BIOMECHANCS, select course 204.
Enjoy

Gum Shoe…. def.
Noun….gumshoe
1. a sneaker or rubber overshoe
2. (slang) A detective or private eye
But in this case……. it quite literally looks like a shoe with gum stuck to the heel and ground ! This pair of pumps is gonna get looks. Pretty amazing what some people think of. Probably courtesy of the guy in the cubical beside you who’s supposed to be doing your mothers taxes but instead is photo-shopping stuff like this to serve his shoe fetish. None the less……a creative mind. We cannot remember where we found this pic……. we would love to give credit to the innovator if he or she is out there…..drop us a line !
By the words of the legendary Rock band Boston………Walk on…..
“Take a look around and tell me what you can see
I guess that all depend on exactly what you want it to be
Is your cup half-full? Is your cup half-empty?
How can you get what you need in the land of plenty?
Everybody gets carried away
Everybody’s trying everyday to remind you
Leave it behind you
What’s it take to see?
What’s it take to believe right from wrong?
Never knowing where you belong
Walk On
Walk On ”


The Tarhumara and Masai Part 2
Setting things straight: MBT (Masai Barefoot Technology) Shoes: Are they really “the Anti-shoe” ?
In the past, many of you have read our articles and opinions on barefoot walking and running As time has gone on you have seen the results of the work we have done for Vibram on their product the Five Fingers (http://www.vibramfivefingers.com/technology/faqs_board.cfm). This Vibram device is the closest to true barefoot walking or running. There are now products in the stores such as the Nike Free and the MBT shoe that over the last few years are gaining popularity. Our job, as we see it, is to report the facts, so here they are.
In 2008 in Outside magazine there appeared an ad for the MBT shoes claiming they are the “anti-shoe, anti-boot, anti-sandal etc”. They imply on their training videos, website and advertisements that this shoe improves posture, protects your knees and tones your muscles, apparently from just standing in them. We think this must be a pretty amazing shoe if it can do all that! However, if your radar is up and working, you should be asking some hard questions before you spend over $230 for a pair of shoes that challenge you each moment not to roll your ankle in the parking lot outside the very store you bought them in. And now, they are available in similar form from Sketchers as “Shape Up’s”, usually for under $100. We say…save your money and invest it in something else, unless you are one of the select few that could benefit from this technology.
Here are some of our major concerns, questions and reasoning for our harsh but sound skepticism.
If you pick up this rather hefty shoe you will notice two things immediately, both of which have concerns. First, the shoe has a rigid last, meaning the shoe does not bend. It has a beveled bottom design called a rocker designed to rock on the ground both forward and backward like a rocking chair. We think Perry put it best: progression of gait over the supporting foot depends on 3 functional rockers.
heel rocker: the heel is the fulcrum as the foot rolls into plantar flexion. The pretibial muscles eccentrically contract to decelerate the foot drop and pull the tibia forward.
ankle rocker: the ankle is the fulcrum and the tibia rolls forward due to forward momentum. The soleus eccentrically contracts to decelerate the forward progression of the tibia over the talus. Ankle and forefoot rocker can be compromised by imbalances in strength and length of the gastroc/soleus group and anterior compartment muscles.
forefoot rocker: tibial progression continues and the gastroc/soleus groups contract to decelerate the rate of forward limb movement. This, along with forward momentum, passive tension in the posterior compartment muscles, active contraction of the posterior compartment and the windlass effect of the plantar fascia results in heel lift.
This shoe takes away from the 3 natural rockers of the foot and means that the foot is not required to do much work other than stand on the platform and let the shoe do the work. In essence, taking it to an extreme, this shoe is really no different than the rocker boot (CAM walker) you might wear on your foot after a fracture, foot surgery or if you have a Hallux rigidus. They are designed to limit mechanical forces traveling through the foot by making the foot quiet, protected and unchallenged by external forces. The rocker boots are designed to reduce heel impact load, and thus induce a more gently rockered mid-foot impact loading, “softening” pronation, which reduces force into the foot. The MBT, at least according to 1 study, lessens heel strike pressure by 11%, but it also diminishes midfoot pressures by 21% and increased forefoot pressures by 76% ! If there is a forefoot deformity, such as a vlagus or varus, this may actualy accentuate pathology, since you are in essence limiting pronation, one of the shock absorbing mechanisms of the foot.
As the studies cite, we agree that they are altering muscle forces through the foot, but is this a good biomechanical change for the the particular foot or foot type involved and should not depend on a shoe to do it for you. More importantly, these changes may have a concerning detrimental side effect; the rigidity of the shoe’s last and its rocker will, in time we believe, weaken the foot intrinsics which are critical for joint protection and stability. The best example we can give are the progressive deformities of hammer toes, bunions and “falling arches” all that result from progressive weakening of the foot intrinsics . This works on the principle of “if you don’t use it, you lose it”.
The second thing you will notice when you pick up an MBT shoe is that the heel “crash zone” (the area that is first impacted at heel strike) is filled with an exceptionally spongy EVA foam, almost as soft as a wet sponge. This “crash zone” is extensive and reaches all the way into the beginning of the mid-foot impact zone. Being the shoe nerds that we are, we can say with confidence that we have never see a shoe with such a soft and expansive rear heel crash zone (not even the Nike Cesium’s (of several years ago) crash zone can compete with this MBT heel zone… and that is saying alot). From what we can tell, this aspect of the MBT shoe was designed to reduce heel strike weight bearing which has some merits, albeit few, particularly in running. When walking, by avoiding heel strike, you are forced to shorten your stride, keep your body mass over the feet and hence reduce the challenges on the pelvis and core in the sagittal plane (these are some of the postural benefits that the shoe claims).
The Masai tribesman (whom the shoe is apparently named after) are a pastoral people who are herders and walk long distances. They ARE NOT runners and often wear simple sandals adorned with beads or sometimes, go barefoot.
If one walks or runs in shoes with a traditional “heel strike” type gait, the cushioning of the EVA heel sole affords a pillow effect, enabling one to “stride out” and achieve heel strike. This is an undesirable trait. At heel strike, there is a deceleration moment of your body mass, this means a shear force on the ground which is why your brain will not allow you to barefoot heel strike when running on a hard, rough surface.
So the question remains: Is the MBT shoe really promoting barefoot biomechanics or is it just using the exceptionally spongy rear crash zone of the shoe which help one to avoid heel strike ? We think the latter. Forcing someone to avoid heel impact/strike naturally forces you to make contact at mid-foot or forefoot (the latter which is bad). For the most part, a midfoot strike is desirable if you have the core stability to withstand this sudden change in gait and posture. Do you really need an expensive shoe to force you to do that when you can make that conscious choice on your own ?
Posture is earned, not forced. Putting a cervical collar around your neck does not earn you posture, it borrows that posture from an external device. The MBT shoes does much the same.
On a positive note, a good use for the MBT shoe is for persons suffering from big toe pain from anatomic (as opposed to functioal), Hallux rigidus/limitus (aka. turf toe) People with limited dorsiflexion of the 1st mmetatarsal-phalangeal joint do well in this shoe since the last of the shoe is rigid and rockered; so the toe does not bend and this reduces pain at the joint. Because of its mass and size, it also makes an excellent doorstop.
The bottom line, if you want to walk or run barefoot, you want to mico-progress into a more minimalistic shoe that bends and gives to motion rather than one which restricts or induces any motion. If trained properly (and there is an exercise progression for the feet, which is specific for each individual) many feet can become stronger and more competent and necessitate less of a shoe. In our experience, inhibiting joint motion and muscular functions over time leads to bigger muscular incompetences, weaknesses and problems that foot intrinsic weaknesses have been known to lead to such as bunions, hammer and claw toes, neuromas and the like.
Parts of this article are from an article we wrote years ago when the MBT’s first became available. As far as we know, we were one of the first on the block to write about them and the above issues. Tomorrow we hope to dig up our podcast we did back then, regarding some of these and other issues….. a little blast from the past, with still great relevance today.
We remain….The Gait Guys…Telling it like it is….
Continuing Education courses we have on the web.
/Goto: www.onlineCE.com or www.chirocredit.com
Biomechanics 201: Basics of Gait (4 hours)
Biomechanics 202: Foot Function and the Effects on the Core and Body Dynamics (1 hour)
Biomechanics 310: Advanced Gait and Running Topics ( 3 hours)
Rehab 117: Lunges, Squats, advanced Squats and Gluteal Exercises (2 hours)
Rehab 116: Advanced Core Stabilization Concepts (1 hour)
Rehab 115: Core activation Training (1 hour)
Rehab 114: Performance Theories and Core Training Concepts (1 hour)
Acupuncture 211: Qi and The Pertinent Pericardium (1 hour)
Acupuncture 210: The San Jiao: a closer look (3 hours)
Acupuncture 209: Points and Acupuncture Points You Should Know (1 hour)
Acupuncture 208: Needle Manipulation Technique (1 hour)
Acupuncture 207: Effects on pain modulation and musculoskeletal function (2 hours)
Acupuncture 206: Homeostatic Points (3 hours)
Acupuncture 205: Needles manipulation, Most common points, and Tongue (1 hour)


Give us your tired, your poor, your huddled….feet!
We are introducing “Footloose Fridays” or “The Ministry of Silly Gaits”. Each Friday we will publish one of YOUR pictures or videos of feet, shoes or gait that YOU send US! They can can funny, entertaining, strange, happy, you name it. Cartoon feet, dirty feet, sexy feet, big feet, the choice is yours. Keep ‘em coming!!
Gait lecture
/Today we are giving a 3 hour advanced gait lecture in a live webinar format.
It is being recorded so that you can watch the lecture anytime you want. Goto onlineCE.com or chirocredit.com
*TeleSeminar Biomechanics 310
Educational Objectives. Following this course, the participant will be able to:
- Discuss the normal walking gait cycle
- Apply the biomechanics of the pelvis and lower kinetic chain during walking to clinical practice
- Predict and discuss problems and clinical strategies that can arise from altered lower extremity biomechanics
- Apply visual analysis skills
- Evaluate case studies in gait analysis
- Clinically apply solutions for gait abnormalities

Not all that glitters is gold… Or The Black Plague Revisited
Yesterdays post discussed our subungual/friction differential of the phalanyx and sock liner theory. A word of caution is warranted, as there is a small chance that the lesion could be something more serious. It turns out that a small percentage represent malignant lesions. http://www.ncbi.nlm.nih.gov/pubmed/21554050.
Know the ABC(DEF)’s of a melanoma. Age (50-70), Black or Brown lesion with 3mm or greater breadth, Change (or lack of) in nail or nail bed despite treatment, Digit most involved, Extension of pigment into the lateral nail fold, Family or personal history.
Don’t believe us, read it here: http://www.ncbi.nlm.nih.gov/pubmed/10642684.
Yup, Black Plague or not, we remain The Gait Guys,


The Black Plague (ok, kinda sort of)……Subungal Hematomas in Runners. Blood under the toe nail. Not what you think it is from !
There are two pictures here, cursor to the right and see the slider that will toggle between the two photos. The photo with bandaid credit given to www.healthandrunning.com the other photo……is a runner client of ours with both a callus pattern on the tip of the 2nd toe and an early small subungal hematoma (read on !)
__________________________________________________________________________
We get inquiries about the black toe nail “Syndrome”……aka…..blood under the toe nails in our runners, and how to avoid them. Lets look at this phenomenon as it pertains to the foot.
This problem has a clinical name, “subungual hematoma”. It means a collection of blood under the finger or toe nail. There are many causes of the subungal hematoma (SH for short as we move forward here). Here are a few, but we have yet to find any good journal articles for one cause that we are seeing as a possible cause…one we will discuss here shortly.
One cause is obvious, the crush injury where someone steps on your toe, you drop something onto it or smash it into something. This is something we have all done at some time.
The most commonly theory of cause is repetitive trauma, thought to be that of repeated impact of the toe into the top or end of the shoe. Heim et al noted this in 2000. This really got us to thinking. Why, when we see these SH’s, do the runners never seem to have shoes that are too short / small or shoe signs of friction (wear patterning) of the toe nail into the top of the shoe’s upper ? Often the runners insist there has been no such contact within the shoe. So we started our own investigation making sure to ask all our runners what they thought and felt as they ramped up their miles in prep for marathons and 20 mile runs or daily doubles, particularly those who seemed regularly susceptible to SH’s. We will discuss our findings and thoughts momentarily, but lets get back to some of the more well known information on SH’s.
The medical literature is full of other types of causes or clues of SH’s that must be investigated, such as medication reactions, autoimmune skin disorders, melanoma, blood disorders (dyscracias or clotting problems). These certainly are not the norm.
It is important to know the anatomy of the area because the nail bed is very rich in vasculature (hence the hematoma creation) and nerve endings (hence the pain) when blood collects in the confined area or it gets torn off from trauma. The nail bed is a derivative of the epidermis containing keratin which gives it its hard nature. The nail grows from a nail root in front of the cuticle and grows distally at a slow but (usually) steady rate. This area is frequently susceptible to fungal infections which destroy the tissue in the area and possibly make SH’s more common.
We will not get into the aggressive treatment of things here because that is 1) not our purpose here and 2) we do not want to be accountable for people getting infections from boring a hole into the nail bed (trephine) to release the blood or the consequences of using plyers to yank it off. We just tend to recommend they be left alone and let nature take its course. (For those bold and tough gang, who chose the plyers method, you should know that there is no fatty tissue beneath the nail and the underlying bone to cushion the area, the nail is the only protection; furthermore you should know that the extensor tendon attachment is awfully close to the proximal nail bed root area !). But when pain it too much, we have our people we refer these cases to. Rather, we tend to look for a cause of the problem.
In a limited number of cases we do see a shallow toe box where there is little room for toe extension, thus the nail can get rubbed on the roof of the toe box repeatedly causing a lifting action of the nail from its vascular bed. This a more plausable cause in our opinion over the “toes hitting the end of the shoe” phenomenon put out there by many sources. Particularly when most people size their shoes sufficiently long enough for the distal foot slip migration that occurs at mid-foot load within the shoe. In these cases a close cropping of the toe nail shoe stop the lifting/friction phenomena on the toe box roof.
However, we seem to be seeing a more frequent trend that we wanted to share here. It seems to go hand in hand with the plague of flexor dominance in our society these days. What we are seeing is a predominance of toe flexion (either a gentle or marked toe flexion ….we sometimes refer to it as toe hammering) in our runners. This just makes sense because of the posterior compartment dominance in runners. (The posterior compartment is made up of the gastroc-soleus complex, long toe flexors and tibialis posterior). So if this compartment is dominant, and there is not sufficient home work to off set the flexor dominance with extensor exercises, then this flexion dominance will continue and possibly worsen. As you will see either in yourself, our photo here, or on the feet of many of your co-runners is a distal “tip of the toe” callus development (usually most on the second toe, and less moving into the more lateral toes) immediately below the leading edge of the toe nail. This callus coincides well with a distal gripping phenomenon of the long flexors (Flexor digitorum longus). So, now imagine, to get the callus there must be repeated friction and since the toe is not hitting the end of the shoe it must be friction into the sock liner bed of the shoe. And if this is the case, the skin is pulled at a differential rate over the distal phalange than the nail bed there will be a net lifting response of the nail from its bed as the skin is drawn forward of the backward drawn phalange (put another way, the callused toe tip is fixed to the sock liner for grip, and then the phalange is drawn backwards from this contact point creating a NET movement of skin forward thus lifting the nail from its bedding). [For an at-home example of this, put your hand flat on a table top. Now activate your distal long finger flexors so that only the tip of the fingers are in contact with the table top. Now, without letting the finger tip-skin contact point move at all, go ahead and increase your long flexor tone/pull fairly aggressively. I defy you to not feel some pressure building under the distal tip of the finger nail as the skin is RELATIVELY drawn forward.] And with the nail bed being so vascular, micro bleeding can occur. This bleeding is slow and takes time. Which brings the big question to light, SH’s seem to mostly occur on very long runs, and never on short runs (where there is not enough nail bed separation repeatedly to create enough damage to bleed, not to mention fatigue of the other toe/foot intrinsic muscles thus necessitating more use of the more powerful long toe flexors.)
There does not seem to be anything out there in the information on this supposition. Maybe we are crazy…….but we do see alot of runners. And once we bring the awareness of the problem to our runners and show them how to reduce the flexion dominance with exercises to gain more extension balance, do we see an arrest of any further Subungal hematomas.
We would love to hear your thoughts and experiences with them, both clinically and as a runner. Let us know what you think about our plausable cause.
we remain……The Gait Guys













