


A cause of ishial pain?
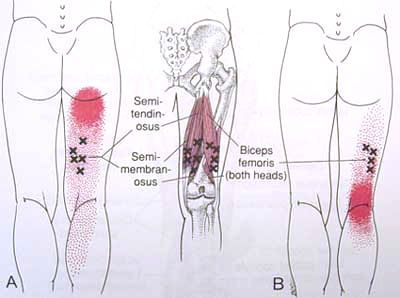
How many of us treat runners on a regular basis? Most of us I would say. While lecturing, I had an epiphany about recalcitrant hamstring insertional pain, that does seem to respond to conventional therapy. Take a look at the trigger point referral pattern for the semimembranosis/ semitendonosis. Note that in closed chain, these are external rotators of the thigh. Thinking about this, they would eccentrically contract (theoretically) to decelerate internal rotation of the thigh (such as with excessive midfoot pronation at initial contact and loading response.
Now look at when these guys fire during running gait. The left side of the graph (up to TO) represents the stance phase of running gait (Mann 1986). The right side represents swing (or float) phase. Note that the medial hamstrings should fire from about foot descent to mid support (or midstance), with a little blast after the foot leaves the ground (asumed eccentrically) to assist in slowing the leg.
Now think about if the foot is a poor lever and remains on the ground just a little longer and rotates medially a little too far (overpronation); this muscle could conceivably be over worked and result in the trigger point referral pattern seen above on the ishial tuberosity.
Ah, but how to fix it?
We could dry needle it and rehab it (better train it eccentrically, since that is how it is working), but it is already overworked, and in my cllinical experience, only provides temporary relief of the symptom. What other muscles seen in the chart could help? Hmmm… Take a look at the tibialis anterior (dorsiflexor/inverter), gastroc (medial) (plantarflexor/inverter), foot intrinsics and glute max/ posterior fibers of the glute medius. All external rotators (save for the foot intrinsics, which should fire from midstance to toe off) and a bonus pronatory decelerator for the tibialis anterior and able to slow an excessively internally rotating lower leg. You better check and make sure they are all on line before just treating the area of the chief complaint!
The Gait Guys. Keeping it real and giving you the tools to do a better job at what we all love to do : ) .













