

Something lighter for Friday Follies.
It just goes to show. You don’t need to be the fastest, just faster than the the slowest guy. Enjoy your Friday!
Ivo and Shawn
Something lighter for Friday Follies.
It just goes to show. You don’t need to be the fastest, just faster than the the slowest guy. Enjoy your Friday!
Ivo and Shawn
The physics of heeled shoes. (or, “Using Newton’s Laws to determine sole pressure.”)
Did you know that a 110 lb. woman wearing stiletto high heel shoes puts a lot more pressure on the ground than a 6,000lb elephant?
First lets begin with Newton’s laws of motion. They are three physical laws that form the basis for classical mechanics. They describe the relationship between the forces acting on a body and its motion due to those forces. They are summarized as follows:
Now, we all know these laws well but here is something a little different today. Today we have lovely Dr. Deborah Berebichez the first Mexican woman at the Stanford University graduating with a doctorate in physics. Here she gives a simple dialogue of the application of these 3 laws to footwear.
In her PhD dissertation physicist Berebichez developed a new method for electromagnetic waves to focus with extreme accuracy in space and time. Berebichez is currently researching at the Courant Institute of Mathematical Sciences of New York University .
Our point ? This is a brilliant woman and so when she speaks about the physics of high heeled shoes, you should listen. 5 inches is the max ladies (oy vay !)
h(max)=Q (12 + (3s/8))
but remember, this the maximum height to stay stable and not risk falling over. It has nothing to do with the risk of pain and pathology to the body that will occur over time ! But that is another mathematical equation that might be best suited for our other favorite fellow-geek and mathemetician Garth Sunden @ Geek Logik who can figure out any formula for anything you wish to assess (for example, “What are my chances in scoring a date with a girl at a bar? click here).
Watch her video attached here to learn about Newton’s 3 laws and how they apply to shoes and heel height. It is great stuff ! It is important to note that even in the highest of women’s heeled shoes heel strike still occurs first (although it is softened as heel height increases……don’t bother asking us how we know this please), hence Berebichez’s point on heel pressure stands correct but somewhat muted. Heel strike does not however necessarily mean true impact. We encourage our patients to note the difference between heel impact and contact. Just because in normal walking gait (running can be different) the parameters dictate heel strike it does not have to be a long latent heavy impact period. Heel strike and impact should not be accentuated, heavy or prolonged. Many gait pathologies can occur when it is significant because the forces move up into the organism, for example increased knee extension or longer duration of the rear foot inversion phase and thus supination foot phase. Rather, begin to focus the thought more on heel contact (sort of a quick kiss as opposed to a long drawn out French-kiss necking session) and the subsequent and immediate soft gradual transition into the full foot loading phases. In otherwords, finesse the heel contact phase. Perhaps if runners had always looked at heel strike this way we would never have seen such a major intellectual epiphany towards midfoot and forefoot strike being the answer and heel strike being the black plague of all things gait/running related. So, at this moment, while it is still fresh in your mind, get up from your chair and walk and feel the difference between kissing the heel on the ground and a major heel-floor make-out session ! You may immediately note the woes of your ways. You may begin to make walking a more conscious finessed movement while in the process begin to note that walking should be soft and fluid, almost an art form or conscious zen-like meditative act where constant awareness is key.
For those new to gait talk and running, remember that walking gait does dictate this heel strike phase where as in proper running this phase is absent when unshod and most of the research is leaning towards this absence when shod as well (hence the minimialist shoe trend of today).
To put a cap on this talk, we would like to say that these are our kinda people ! Geeks rule ! (but then there are these kinds of people here (Las Vegas high heel shoe race, for those of you who don’t want to link elsewhere) that need to have their heads checked a little…… have they not hear Dr. B’s lecture on heels ?)
Shawn and Ivo…… The Gait Geeks, the guys you beat up in grade school, and now the kinds of geeks you gravitate to for intellectual stimulation. How ironic huh ? Who’s your daddy now !
more on Dr. Carrick
you will see here some clues into what Dr. Carrick (One of Dr Ivo’s and Dr Shawn’s Mentors), and what we, look for in gait and arm swing etc. It is so much more than telling someone to swing an arm more, or turn a foot in. It is about the brain and global function. Remember Dr Ivo’s Neuromechanics lecture on the central integrated state? (if not click here). That is what this is all about.
Neuromechanics Weekly:
What does the Reticular Formation have to do with gait?
Have you ever worn flip flops? What do you need to do to keep them on? Clench (flex) your toes (specifically your flexor digitorum and flexor hallicus longus). What does that have to do with gait?
Take off your shoes (hopefully you showered); reach inside (unless there is something growing in there) and pull out the removable insole. Look at it. See those toe marks? Looks like someone has been clenching their toes again! So what?
This video exemplifies why flexor dominance (you have heard us say it many times) inhibits extensor activity. The upper part of the reticular formation fires the extensors, but the lower part inhibits them AND the corticospinal tract (basically the motor pathway you use to fire most of your voluntary flexors) stimulates the lower reticular formation (which inhibits the extensors). Many pathologies are because of flexor activity, and his is one of the pathways that’s facilitates that pathway. The key to fixing many problems? Fire the extensors! (And stay out of flip flops)
The Gait Guys….figuring it out and explaining it to you in terms that make sense. And no, we do not own any flip flops….
Vitamin B12 deficiency: Another cause of Gait Ataxia.
Here is where our clinical background gives us another slight edge on those in the gait and movement fields. Once again we need to bring to the table another cause of gait problems. This problem can manifest as a gait, running or simply a mild impairment of muscular coordination patterns. There are so many people out there these days providing “care” to athletes and those that want to stay physically fit. Many of these care givers however are not in the medical field. They might be a coach, trainer, massage therapist, physical therapist, or God forbid someone you are taking advice from over the internet. The problem in giving health advice or treatment is that it is easy to do and often, if you are without a medical license, fraught with the “you cannot be aware of something that you do not know exists”. So, if you are one of those who trains or coaches people, offers nutritional advice, stretches, massages, “activates” or uses other means without a medical license, you had best be aware that you could be missing things. And, even if you do have a license, failure to get results is sometimes a result of something being missed diagnostically, not a failure to treat enough or not using the right techniques or therapy. This is not a dig at anyone or their passion, it is just a fact, without a medical background you just might not be exposed to the gamut of things to be aware of. Thus, it is quite possible that “interventions” are not working because other things are lurking below the surface, things one just might not be aware of. On this note, It is never a bad idea to ask your athlete if they have had some blood work and chemistry workups in the last 12 months, especially if they are not progressing or are having some of the early subtle signs or symptoms of something bigger lurking systemically. Read on.
You will recall from our last talk on movement impairments from organic or systemic nutritional complications (Nov 10th, Gluten Gait Ataxia) that there are several metabolically driven gait and ataxia disorders. The one we are going to talk about today is Vitamin B12 deficiency ataxia (we are going to downplay the pernicious anemia thing for now to stay focused).
You will recall that the definition of ataxia is pretty broad. Ataxia refers to an inability to coordinate bodily movements, especially movements of the muscles. Thus ataxia can manifest as a possible aberrant motor pattern, lack of coordination or subtle gait impairments such as early balance difficulties.
Vitamin B12 (aka cobalamin) is a water soluble vitamin that has a paramount role in the normal function of the central nervous system and blood formation. It is one of 8 B vitamins. Vit B12 deficiency is nothing to shrug off. In its most severe unaddressed form it can potentially cause irreversible central nervous system damage (for you doctor-types out there you will fondly recall the long lectures on SCD (subacute combined degeneration of the spinal cord and CNS) from your favorite neurophysiology professors). At subacute B12 levels softer symptoms can range from fatigue, depression, dizziness, memory loss, confusion, anxiety and other neurocognitive problems as well as altered executive function, ataxia (unsteady gait, balance impairment) peripheral limb or circumoral numbness or tingling. The vagueness of these symptoms often lead to untimely diagnosis.
Vitamin B12 occurs naturally in most animal products, but if you are one of millions of people who cannot absorb B12 efficiently, then you can begin experiencing symptoms of vitamin B12 deficiency. And yes, to remind you once again, the symptoms are soft and vague at the start. They are vague because it takes time for gradual degradation of the nerve’s myelin sheath, the place where Vit B12 has its impact. It is this myelin, the conductive coating on a nerve, that is necessary for accurate and timely communication between the central nervous system and muscles and organs. And it is here that gait ataxia truly begins. The nerves of your spinal cord rely on a steady in and outflow of information from your nerve sensors throughout your body. Messages to and from the nerves in your limbs are conducted along the spinal cord (particuularly in the spino cerebellar and dorsal column tracts: See Dr Ivo’s neuromechanics lectures for a review of these here ) and to the brain, thus controlling gross and fine motor tasks such as running, walking, dancing, climbing, skipping, or tapping your feet. Nerve damage causes these signals to become misinterpreted, resulting in poor coordination, or gait ataxia.
Here are some signs and symptoms of gait ataxia:
So that is our little talk on gait ataxia and its relation to Vit B12. It is a quite in-depth topic to be honest but we want to keep this concise. In terms of recommendations, we are not going to make any here today. The recommended daily allowances are easy to find on the internet. Two things you can do, you should improve your diet (we all can) and get yearly blood work studies. If you are vegan (unless you are a lacto-ovo vegetarian) or do not consume much in the way of animal based food products you need to consider B12 supplementation (that or start eating termites - B12 rich !). You should also be aware that there are many things that can alter Vit B12 absorption /integration such as birth control pills, alcohol consumption, nicotine, medications, antibiotics and many others. These are consumables that increase your risk of B12 problems and thus risk for gait ataxia and the other B12 related issues. Most of the time, ataxia is a difficult diagnosis to make (unless a copious single event of alcohol consumption at the local pub is the culprit).
Bottom line. There is so much more to Vitamin B12 deficiency but this was not meant to be that forum. Ataxia and gait alterations are nothing to dismiss, especially in the elderly. There are many causes of ataxia and this is just another that we wanted to bring to light. The nervous system and muscular systems have some definite source needs and Vit B12 is one of them. Without the right fuel these systems will begin to show impairments, soft impairments at first which could be the difference in a high level athlete’s performance. If your parents, patients, athletes or those you know are expressing some vague and subtle symptoms, educate them. Better yet, send them off to their doctor if symptoms persist, rather than handing them a bottle of Gatorade and casually telling them they are probably just dehydrated, anemic from low iron or low on electrolytes …. as it so often occurs.
Shawn and Ivo, The Gait Doctors
On Sunday over 700 people received our weekly newsletter “The Week in Gait”.
This newsletter is for those who have emailed us requesting to be signed up or have opted in through our Constant contact app on our Facebook page (that is the easiest way for you and for us).
If you want exclusive content not on the blog or facebook, if you want first hand notice of a lecture we are giving, a magazine article in the works, an early bird DVD release (yup, on their way in early 2012), or just want a nice recap of the best blog posts of the week with some extra exclusive commentary from Shawn and Ivo……. then you want to be receiving our weekly newsletter….. The Week in Gait.
Sign up today or email us. The newsletter will go out every weekend, at least we anticipate that being the case.
Shawn and Ivo
Lauren Fleshman on her injuries. Biomechanics you say ?!
We should have called this blog series, Saving Lauren Fleshman.
She seems like a real smart gal. It is not her job to figure this stuff out though so we do not fault her in the least. We just hope she or her doctors look at our blog posts and youtube videos. Anyone want to nudge her in that direction ?
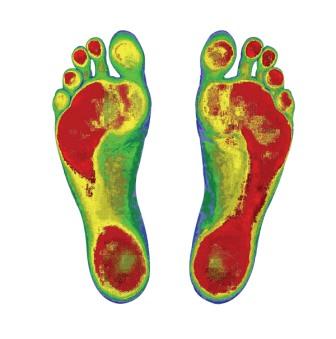
Foot Scan: A Case Study.
What can we glean about this person from this pressure sensitive foot scan ? Remember, no examination possible here so lets see what we can assume is happening. These kinds of mental aerobics help keep us clinically sharp and help us pick out subtle patterns in someone gait when we do gait assessments …. so that we can prove them or disprove them on the table during our exam. Remember, for this case, the person is standing, not moving through the gait cycle like in a normal pedograph mapping or F-Scan (hence making an orthotic or true and accurate assumptions from this type of static scan would be really silly … but alot of people and companies do it ! Sadly.) We are presenting this case for the means of mental stimulation and observation only.
Hope this was a nice little exercise in observation and mental juggling.
By the way, Juggling is a great mental exercise….. A Princeton researcher, Les Fehme suggested we can optimize our overall performance in life by broadening our focus. Juggling is one excellent way to do that. He claims most people have a narrow focus, a lack of awareness of their own body sensations or emotions. A recent CNN report suggested juggling increases the amount of grey matter in areas of the brain that process and store visual information, proving what was not thought possible – that new stimuli can alter the brain’s structure. A comparison of brain-imaging scans of non-jugglers and other volunteers before they learned to juggle and three months later, revealed an increase in grey matter in certain areas of the newly trained jugglers’ brains.
And so … thanks for juggling with us today. We hope you did not choose to use chainsaws or Ron Popeil knives (“Wait, there’s more! We’re going to double your order!”). Wanna get a little crazy driving more brain grey matter integration ? Try running while juggling, if you dare ! We recently heard of a guy that broke a record running a recent marathon juggling 3 balls the entire time. Who has time for this shenanigans ?! We have troubles getting our laundry done.
Ivo and Shawn ….. your jugging court jesters. Jester, hmmmm … perhaps a good label for us. Sounds like it was a fun job.
(define: A jester, joker, jokester, fool, wit-cracker, prankster, or buffoon was a person employed to tell jokes and provide general entertainment. Jesters are stereotypically thought to have worn brightly colored clothes and eccentric hats in a motley pattern. Other things distinctive about the jester were his laughter and his mock sceptre, known as a bauble or marotte.)
Oscar Pistorius……..here on Inspirational Sundays on The Gait Guys.
From the article,
“The big problem created by wearing high-heel shoes was abnormal weight distribution, she said. Instead of the foot bearing the weight of the body in the heel and the ball of the foot, all the weight fell on to the ball of the foot when wearing high heels, especially narrow, pointy-toed shoes. The increased pressure could make corns and callouses develop on the ball of the foot, increase the likelihood of developing ingrown toenails, bunions and hammertoes and contribute to neuroma, a painful thickening of the nerve between the toe bones. In some habitual heel wearers the calf and Achilles muscles could shorten into a tighter position leading to strain and an increased risk of tendonitis or tendon rupture when reverting to walking in a flat shoe or barefoot. Foot problems typically started to present for women in their 40s, with pain limiting their ability to function, she said. "Most foot conditions are chronic and develop over a period of time,” Professor Bower said. As we age our joints, ligaments and tendons loosen and the foot will lengthen slightly and incrementally because it is no longer toned. The fat pad under the heel and ball of the foot that cushions the foot from birth declines and the bones and joints become more prominent. The older foot, with less naturally occurring support and padding, was therefore at an increased risk of problems from wearing high heels, she said. “
It is all stuff most of us have heard already, but it is always nice to hear it again and pass it onto our patients and children.
High heels and women in them are great to look at, but just not meant to walk in for any extended period of time. The Gait Guys say, "Put them on your fireplace mantle where you can enjoy them daily, rather than on your foot.”
Ivo and Shawn, The Gait Guys
Friday follies….. not exactly gait related. Not sure if we shared this one in the past but its worth it to enjoy a second time !
We can put some “alternative” exercise stuff up once in awhile can’t we ?
we almost wet ourselves on this one….. sledgewand ! Snakeshaker ! Pink socks !
Rock on Ben, rock on dude !
Enjoy
Here is a little trick we use with our runners…… stop running on the track in your lane between the lines…… start running ON the lane line….. put your body over the lane line but do not let your feet touch the line……run on either side. You will feel choppy at the start but you should feel how much more glute and abdominal use and support you need. Start with 20-40 meter runs and build up. Once you are good at it, you can run anywhere and just imagine the line !
How a really fast runner could potentially be faster, and less injured. A 2nd look at the amazing runner, Lauren Fleshman.
Here, as promised, we take a closer look at talented runner Lauren Fleshman from our 11/22 post. Remember, we are not being critical,
our posts are never meant to be critical or inflammatory, only calling things the way we see them from the information we can glean from the videos we see or that you send. Remember, our dialogue is rarely from hands on clinical examination to prove that what we see is factual and not an assumptive compensation pattern that is so often seen on video (we have mentioned this on many older posts). Yes, video analysis shows compensations, as you see here with Lauren. What you see is often not what you get, but it is critical information that helps drive a logical path towards educated assumptions that can help lead to an accurate diagnosis. The two Gait Guys, with nearly 4 decades of clinical experience, have done the ground work necessary to make many of the assumptions we make. But we are not always right, so take our posts as solid, experienced and quite often research-backed learning information, and get to see a skilled gait neuromuscular specialist like us to pound out the definitive diagnosis.
We believe Lauren could run faster. Here we offer our experienced thoughts on what we did to help athletes with mechanics just like hers. After perusing Lauren’s blog and looking at the history of her injuries (namely navicular stress injurires, and hip problems) our post from Tuesday Nov 22 seems pretty “crystal ball” spot on.
Lets go back to the video and watch the right foot strike from:01-:02 (yes, you will need to stop the video and start again a few times. What do you see? A right foot coming down to the ground in inversion viewed as a sharply pitched lateral foot strike. This is brought on largely by her troubled mechanics of a cross over gait but it can also be due to internal tibial torsion and a forefoot varus, as they often occur together and may be part of her clinical picture. Immediately on strike you see the midfoot collapse and the foot abduct (progression angle increases) BUT the knee holds steady, due to her most excellent glute max strength. This sudden midfoot pronatory collapse and the sudden violent abduction of the forefoot will force the navicular bone medially (adduction and medial rotation to be exact) and is very suspect to her navicular injuries in the past. Fixing the cross over biomechanics will have a huge impact on reversing the sudden and aberrant loading of the medial foot anatomy.
Now watch at :03-:11; the left foot. What do you see? An adductory twist of the heel. Thomas Michaud calls this an “abductory twist” in his landmark book “Foot Orthosis” but we are talking about the same phenomenon here, it just depends on your point of reference. Our reference is the heel moving medially, or adducting as you see here in Lauren’s video, so we will use the term “Adductory twist” at least in this post. Lauren’s adduction heel twist is greater on the left than right and occurs with and MORE apparent pronation. According to one interview we watched (link click), she has had multiple stress fractures on this left foot. Hmmm… Looks to us like she could have some mild bilateral internal tibial torsion (knees point in when the the feet are straight; notice how the Left knee looks straighter and the right is always pointing externally; :06-:14) and possibly some mildly increased tibial varum on the left. Perhaps she has a Right short leg, possibly functionally short as opposed to anatomic, and this can come from asymmetrically impaired hip rotation mechanics. Her injury history is suspect. This seems supported by the subtle Right torso lean (:16-:22) and Left hip hike you see during Right stance phase (:22). A functionally longer leg, more varum, more visible pronation, internal tibial torsion: it adds up to a stiffer lower extremity which would absorb more force. We wonder which Nikes she runs in….
So, what to do?
We can’t change her torsion or tibial varum if they in fact exists, examination is always conclusive, not video clips (unless you have seen the movie “Gattica” then fixing them is a distinct possibility).
If she does have a Right short leg, we could lift it, beginning with 2mm sole lift. But we would have to prove that it is anatomically short first. Regardless, sometimes temporary use of a sole lift helps restore some symmetry. It it is functionally short, from impaired hip rotation for example, we could start there with short term help of a lift. But, remember, if you can resolve the functional pathology, use the lift like an orthotic should be used. Meaning, a therapy device to temporarily help someone achieve proper skill, endurance and strength (our mantra) so that the device can be weaned out of.
We could work on her suspect forefoot varus (if it exists, it is nearly impossible to tell for sure in a video clip with shoes on), by increasing mobility of her 1st ray (see our Video here ) but we would first fix these cross over gait mechanics with these video skills (click here) and then see how much varus is expressing itself as pathologic mechanics.
Her chiropractor seems to be doing a great job maintaining mobility. It would be great to look at her intrinsic muscles of the foot; we suspect she has a weak EHB (extensor hallucis brevis) if a forefoot varus is present, among other things.. We have seen photos of her feet on her great blog and she is getting alot of distal callus formation on her toes (if that was in fact her foot) so we suspect she is over dominant in the long toe flexors (which pairs up nicely with weak EDB and EHB). This might suggest further intrinsic foot muscle weakness, examination muscle testing would be necessary of course.
Those are some ideas of places to start. Stabilize the foot from below and hip from above and something better has to come out of this. If we knew more, we could give you more. If you know her, have her drop us a line or head to her blog and suggest she peak at our work. We would love to help this truly amazing runner. We love to see great athletes perform at the top level. Mostly because we are in awe and jealous of what they can do and what we cannot do, and more so because we always wonder if what we are good at will make them faster. It is what we do.
* A big thanks goes out to Lauren and Nike for posting this video and for being a good sport (we hope) about our evaluations. Thanks for being such a great athlete and for being slightly less than perfect. There is nothing to learn from being perfect and no room for becoming greater at your craft. No one wants to take their medicine when it tastes baldly, and so we work on staying healthier. Only from suffering the humblings that come from the watchful scrutiny of being one of the best can we become aware of our flaws and triumph over them.
The Gait Guys…two foot geeks promoting foot and gait education. No gait is safe….
Ivo and Shawn

Shoe Fitting is about to get smarter.
Here is some news on our new shoe fit program for 2012.
Go ahead. Click on the picture. You know you want to : )
Random thoughts on gait (and other) motor patterns …….
It is quite possible and reasonable to assume that a motor pattern is a natural mechanism for joint and multi-joint protection. Consciously trying to alter a motor pattern is likely to drive an improper pattern or one that is deemed unstable by the brain.
Scenario: client has right foot spun externally into the frontal plane by 15 degrees more than the opposite side.
In this scenario, this could be the reason why merely attempting to turn inwards a right foot that has drifted its way in time outwards does not hold even though it is clearly a deviation from symmetry. It is likely the fact that the brain, in such a scenario, has calculated that there is not sufficient stability in a more neutral symmetrical foot progression angle and thus has found the necessary stability in a more turned out position. As we have always said, subconsciously turning the foot outwards helps to cheat into the frontal plane, likely because that plane is less stable with a neutral foot and with the foot “kickstand” turned out, stability is achieved. Thus, engaging the foot better in that plane gives the brain and body the perceived and actual stability that it feels it needs to more naturally provide joint or multi-joint stability. That is not say this is optimal biomechanically for best-case function, but in this picture with all the parts assembled in their present functional ability, this is the optimal pattern. It is however fraught with risks and probable consequences, and these are what may play out in time to develop into an injury. It is safe to say that the central nervous system (brain etc) will only allow one to place the body and its limbs into positions of perceived stability. We say “perceived” because there are parameters that can fool the brain. For example, the peripheral neuropathy numbness and loss of proprioception from advancing diabetes can lead to faulty input from the peripheral sensory receptors thus procuring a miscalculated decending motor pattern, and possible placement of the limb in a less than optimal position. Do not be mistaken, the brain thinks this is an optimal limb placement, but it does not know it did so on faulty sensory information. The brain assumes that the information is accurate. This is why you see such horrible fragmented unstable and waivering gait in advancing diabetics. Their feet can get so numb that there is simply insufficient sensory information to develop any semblance of a clean gait motor pattern. The same goes with an ACL deficient knee. The ACL is a major proprioceptor, a major driver of joint position sense. It is not nearly as detrimental to the motor pattern as advanced peripheral neuropathies but it has a similar effect, just muted. And in many cases this can be worse. In a high level athlete, this possible lack of obvious awareness of key proprioception / joint position sense can let the athlete get into a potentially dangerous loading position where the joint is at higher risk. Where as a full blown neuropathy patient knows that such a task is impossible.
Just some random thoughts…….. internal cortical ramblings of gait crazed madness.
Happy Thanksgiving everyone !
Shawn and Ivo
We were recently asked by Kara Thom to write a brief description of the perfect running shoe. For 20 years Kara has been writing about running and triathlons while pursuing the sports herself. She is the author of Hot (Sweaty) Mamas: Five Secrets to Life as a Fit Mom (Andrews McMeel, 2011), Becoming an Ironman: First Encounters with the Ultimate Endurance Event (Breakaway Books, 2001), and the children’s book, See Mom Run (Breakaway Books, 2003). She is also a Runner’s World reporter.
* Embedded in her article is our description of “the Perfect Shoe”. Enjoy her great piece.
Ivo and Shawn
Don’t let the title scare you. While watching this excerpt from an acupuncture lecture, think about the implications for gait.
In this installment of Neuromechanics weekly, we discuss how everything we do, smell, see or hear influences muscle tone through the cerebellum. The take home message is environmental cues as well as therapeutic ones will influence muscle tone via the muscle spindles..
You just can’t get away from neurology. It is EVERYWHERE!
Gait Video Analysis: Olympian Carl Lewis.
Carl Lewis: arguably one of the great runners of the 20th century, especially in form.
Today we are going to use this video to look at a few specific components.
First, lets compare his front on technique to Lauren’s from yesterday. Notice the total lack of limb cross over? Lauren showed almost a “running on a line” where as Carl is running on two lines. This requires more gluteal strength, and if you can get to a position to train it you can make it stronger. You will also notice that with Carl’s reduced cross over the tibia are vertical and the degree of foot pronation is minimized thus affording less time in the dampening pronation contact phase in comparison to Lauren.
Now lets talk about the gluteus maximus for a minute. The function of the G.Maximus is multifactorial. The G.Max is mostly silent at low activity levels such as level and uphill walking, but it increases substantially in activity and alters its timing with respect to speed during running.
The G.Max controls trunk flexion on the stance-side and it contracts in the late swing phase (when the leg is finishing it’s swing in front of our body) through early stance phase to decelerate hip flexion and initiate hip extension. There is lessening gluteal contraction at toe off but the medial bundle (more sacral divisions) offer a brief burst of force. So, if you look at its activity levels and the timing of them, you will get the distinct sense that the gluteus maximus function is to pull the leg through hip extension. The key word here is PULL. Remember, the foot is fixed to the ground in the stance phase. So as the glute fires in the early half of stance phase, when the hip is still in relative flexion, it pulls us through the stance phase thus driving us forward. Mind you, the core must be strong enough to hold the pelvis static so that the extension can occur through the hip and not travel upwards to create lumbar extension. You can get a great sense of this in Carl Lewis’ video above. Many people see the G.Max as a push off muscle but this is not true. It is more of a pull muscle, pulling us forward on the ground as opposed to pushing us forward .
Want to do some precision work to focus on the feeling of the glutes “pulling you through”, then try some hip-glute extension pull throughs (click) with a cable crossover on the bottom setting or heavy kettlebell or sandbag swings (click). Best of all to get the feel of what the glute max does …… grab a skateboard and plant one foot on the board and begin pulling yourself through the stance phase with the leg…..after all that is what you are doing, pulling yourself through. Of course form is everything, so be careful and focus on slow movements that are clean and precise. Just do one thing when you do either of these. Feel the foot contact and imagine the hips and glutes driving forward on a stiff protected core while you feel the posterior drive through the foot. This is likely the feeling Carl would be aware of in his feet at the 10-15 second mark in the video.
Some readers will jump at the opportunity to say “hey, Carl is a sprinter, Lauren is a distance runner…… you cannot compare apples and oranges !" Our response here is , yes that is correct. But they are not that different, look at the kick in the end of close a distance race…..are they really that much different ?" But what we really need to say here on that question is, "That was not the point of this exercise. We are looking at flaws here." If we asked Lauren to sprint, we would see the same pattern as in her video here.
Shawn and Ivo………. just a couple of nerds always wondering why everyone else is in the box and we are standing outside of it. It’s not fair.
The Cross Over gait in a professional runner.
This is Lauren Fleshman (born September 26, 1981) is an American track and field athlete. She was the U.S. 5000 meters champion in 2006 and 2010. In the 5000 meter final of the 2011 IAAF World Championships[1] she finished 7th place, equaling the highest ever finish by an American woman in that event. She debuted in the Marathon November 6, 2011 at the ING New York City Marathon, finishing 12th. She currently trains in Eugene, Oregon as part of the Nike funded professional team Oregon Track Club Elite.
__________________
What the Gait Guys have to say. First of all, this isn’t meant to pick on Lauren, we are big fans of hers. Her amazing numbers are evidence of her dominance. We still think her best days are yet to come, and we hope this offers a means to such an end.
This is a great video depicting what often happens at the foot level because of the angle of impact in the cross over gait. Maybe she should watch our 3 Part series on Cross Over Gait (here is Part 1,click). With all that excessive pronation at the foot we suspect there is more gas in the tank in this already amazing runner. What we like is that at the pelvis level (relatively, she has a small hike on the L during R stance phase; look at :22) it is apparent that she has sufficient abdominals (particularly obliques) and gluteus medius strength to avoid the contralateral hip drop during single leg stance (the gluteus medius and gluteus minimus function together to pull the thigh away from midline, or “abduct” the thigh. During gait, these two muscles function principally in supporting the body on one leg, in conjunction with the tensor fascia lata/TFL-ITB, to prevent the pelvis from dropping to the opposite side).
The video also shows no evidence of frontal plane pelvis shifting (see our 3 part videos) which are often seen in the cross over gait and the knees are not giving into the valgus stress created at the ankle from her collapse. So our question is, why doesn’t she get out of this power-leak style so she can be even faster? Sure you could argue, as many do, that if it ain’t broken don’t fix it but from our perspective why not make it better?
Her foot pronation is clearly excessive from driving her power down through an angled tibia instead of driving down through a vertical tibia. This angle of attack is obvious, look at the significal lateral foot initial contact, her foot motion is lateral to medial, not sagittally forward. She is wasting energy because her foot is spending more time moving lateral to medial than forward. She is plenty strong, as evidence by the knee not passing midline into valgus (the glutes are not only extenders but external rotators). She does have one heck of an abductory twist (watch that rear foot at heel rise, yikes! We wonder if her achilles are sore after a long run!). This is surely limiting her gluteal availability. This is just not efficient biomechanics. The longer the foot has to pronate the less time it has to supinate. Our greatest power is in push off from a fully supinated rigid lever foot, not one that is still coming out of pronation. Remember, the glute is going to power through that foot, why not get it positioned optimally do take the glute on and utilize the glute as much as possible ?
In time it could catch up to her in the form of injury, we certainly hope not. We realize this is already a champion runner, she has the numbers to prove it, but why not do what is necessary to become untouchable ? We hear it all the time, “I am injury free, why should I address it?”. Our answer might be, “then why bother doing routine car maintenance if it is running fine or yearly blood work if you feel fine ?" Why do you think NASCAR pit teams and mechanics do all the work they do ? Because they want to go faster. This is such a simple fix. We think she could be so much faster.
Tomorrow we will show a video of Carl Lewis, arguably one of the great runners of the 20th century, especially in form. You will not see a step out of place let alone a cross over. So we will see you tomorrow for that piece.
Bottom line … . Our guess is that the main reason Lauren has not fixed her cross over is that no one has brought it to her attention … until now. In a future post, we will discuss some possible fixes as well.
The Gait Guys ….. Just two guys not trying to upset anyone, just trying to share what we know, what we do everyday, making fast people … faster.
Happy Thanksgiving everyone……. from us both……. Shawn & Ivo

Donate here











Help keep us free ! Make a donation by clicking. here.

Donate to get exclusive content from The Gait Guys
OUR SEARCH BOX IS INTUITIVE, TYPE IN YOUR KEY WORD, WAIT, THEN SCROLL DOWN.
Email us: our email is found under the "Disclaimer" Tab above.

Powered by Squarespace.