

The Beef on the EDL.....
/We have long been promoting appropriate function of the long extensors of the toes here, in our practices, our lectures, on Youtube, in our book......You get the idea. Lets take a closer look at this often weakened and overlooked muscle.
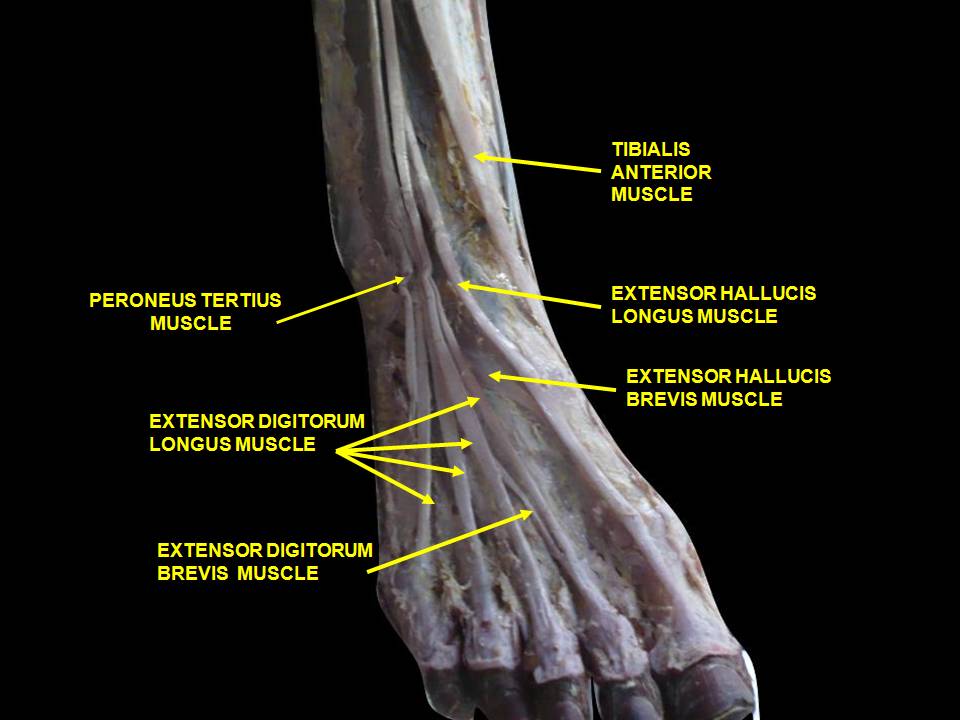
We remember that the EDL lies mostly in the superior and somewhat lateral part of the anterior compartment of the lower leg, comprising approximately the upper 2/3 from under the lateral tibial plateau and fibula, and from the interosseus membrane. It lies under the tibialis anterior, and the extensor hallucis longus lies below it. Its tendons pass inferiorly and travel under the extensor retinaculum and attaches to the base of the distal phalanges of toes 2-4. These muscles act from initial contact to loading response to help eccentrically lower the foot to the ground and ensure smooth heel rocker and most likely attenuate the speed of initial pronation as the talus glides anteriorly on the calcaneal facets and again from terminal stance through initial swing to provide compression of the metatarsal phalangeal and interphalangeal joints, to offset the long flexors (which are often overactive) and create clearance for the toes during swing.
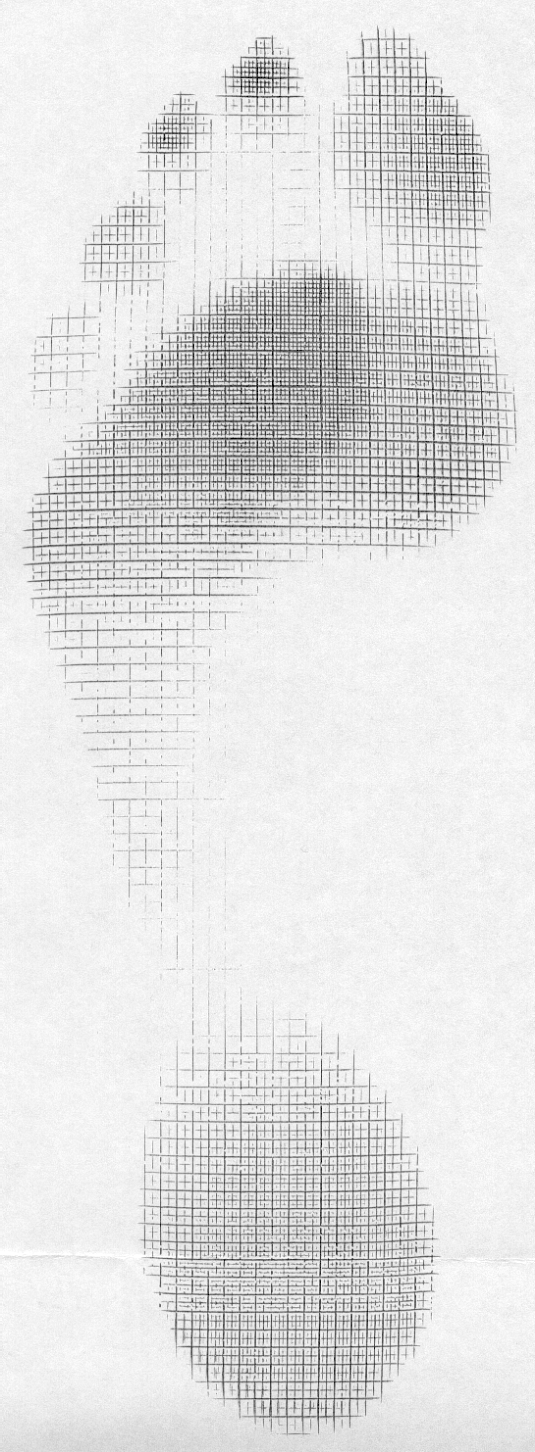
What does it look like when the long extensors don’t work so well? Have a look at the pedograph on the right (pair J howard r). what do we see? First we notice the lack of printing under the head of the 1st metatarsal and increased printing of the second metatrsal head. Looks like this individual has a forefoot supinatus, or possibly a forefoot varus (cannot get the head of the 1st metatarsal to the ground, and thus a weak medial tripod, possibly insufficient extensor hallucis brevis, peroneus longus, flexor digitorum brevis, or all of the above). Next we see increased printing of the distal phalanges of digits 2-4. Looks like the long flexors are dominant, which means the long extensors are inhibited. What about the lack of printing of the 5th toe? I thought the flexors were overactive? They are, but due to the supinatus, the foot is tipped to the inside and the 5th barely contacts the ground!
How do you fix this?
- Help make a better foot tripod using the toe wave, tripod standing and extensor hallucis brevis exercises.
- Make sure the articulations are mobile with joint mobilization, manipulation and massage.
- How about dry needling and acupuncture to improve function?
- Make sure the knee and hip are functioning appropriately.
- Put them in footwear that will allow the foot to function better (a less rigid, less ramp delta shoe).
- As a last resort, if they cannot make an adequate tripod because of lack of motivation, anatomical constraints or both, use a foot leveling orthotic.













