

Something a little different for a change: Case Management of a Post Surgical Foot
/


In this series, we will follow the progress of a post surgical, post rehab foot. These are the actual case notes and you can follow our thought process as we move along.
History:
JM presented with left-sided content foot pain. On July 24 she broke her left navicular and cuboid (pretty unusual, as these fractures are rare. Navicular fractures are usually stress fractures (1), occurring in about .6% of fractures in one study (2). Cuboid fractures are also rare and occur in less than 1.8 per 100,000 (3) ) She also tore the reticular ligaments. this happened when she fell down the stairs, inverting and plantar flexing the foot.
She has had extensive physical therapy as well as plate fixation of the navicular but is still having constant discomfort; she feels a pinching and shock like sensation in the right arch, particularly when loading the foot (whenever you hear about a "shock like pain, begin thinking about nerve related pain). She has been on gabapentin in the past which helped but she stopped it 3 weeks ago with no regression of her symptoms. She feels frustrated.
She was in physical therapy until the end of December. She has continued with exercises consisting of plantar flexion/toe raises, mobilization and inversion/eversion, squats/lunges as well as massage. She has improved but not completely better. She is able to hike 4-5 miles with little pain (boy, those Colorado women are tough!). The foot generally feels better with non weight bearing and rest as well as avoiding impact. The foot feels stiff in the morning and she limps for the first 10 minutes after getting out of bed. Most recently she has had x-rays at VSO with Dr. X.
What did we find?
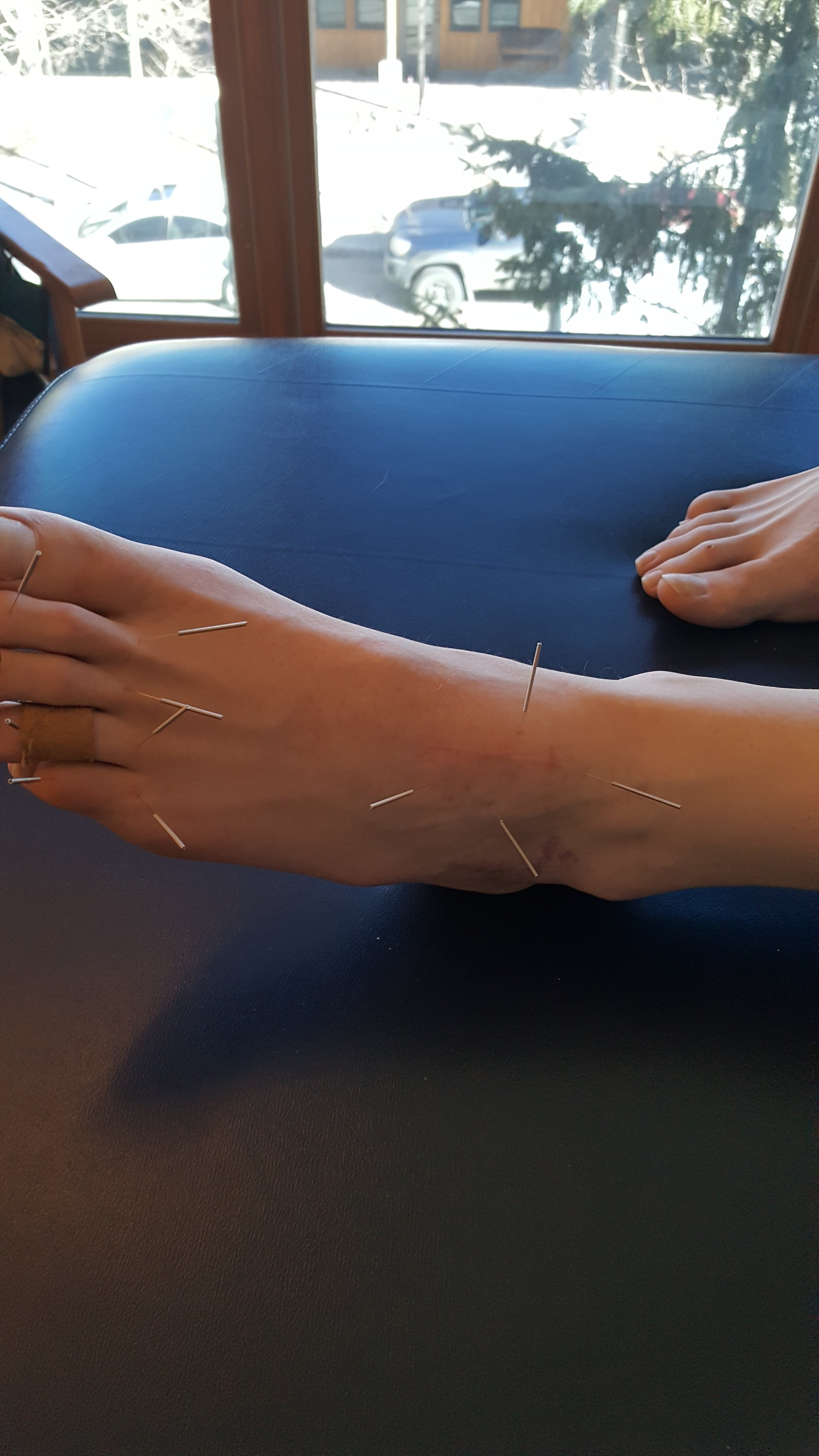
There was swelling noted over the extensor digitorum brevis with significant weakness of it as well as the extensor longus. No sensory deficits, reflexes intact. She had an anatomically short left short leg which appeared to be functional. There was a scar visible over the dorsum of the foot approximately 2 inches in length (see photos) and some discoloration lateral just anterior to the lateral malleolus. palpation along the medial plantar nerve revealed increased sensitivity below the navicular and into the medial heel.
She has external tibial torsion bilaterally and limited eversion of the forefoot on the right. Her cuboid was moving appropriately but talonavicular articulation was not. She has adequate hip extension, 15+ degrees and ankle dorsiflexion bilaterally in excess of 15 degrees.
One leg standing with eyes open was less than 10 seconds. Loss of flexion and extension about the L SI joint.
no x rays available for this visit
What we think was wrong:
Left foot pathomechanics (talonavicular) secondary to surgery and fracture. She has significant weakness of the short and long extensors as well as limited eversion and proprioceptive difficulties.
Discussion:
The talonavicular articulation is one of the key joints in mid foot pronation. Pathomechanics appear to be compromising the medial plantar nerve. This is exacerbated by her inability to fully evert the forefoot and pronate through the mid and forefoot (pronation is dorsiflexion, eversion and abduction).
What We did:
We manipulated the sacroiliac joint and metatarsophalangeal articulations. We held off on any mobilization of the foot until we see her x-rays, hopefully available next visit.
We treated with neuromuscular acupuncture at the origin/insertion of the long extensors as well about the short extensor mass where the swelling was located. She was given the tripod standing, lift spread reach, toes up walking, and tiptoe waiting exercises to perform 2-3 times daily. She is scheduled for followup next week with x-ray review.
1. http://emedicine.medscape.com/article/85973-overview
2. http://journals.sagepub.com/doi/pdf/10.1177/2473011416S00299
3. http://www.uptodate.com/contents/cuboid-and-cuneiform-fractures













