The effects of aging on the proprioceptive system
/When the nervous system breaks down, there are predictable patterns that we can see. Aging isn't that much different in the grand scale of things than some neurological disorders. Here is a brief video of a gentleman that presented to us with neck discomfort and limited range of motion. Step through it several times before proceeding.
Hopefully, you noted the following:
Increased arm swing on the right (or, decreased on Left)
Pelvic shift to the left on Left stance phase
Decreased step length on the left
Hip hike on Left during Right stance phase
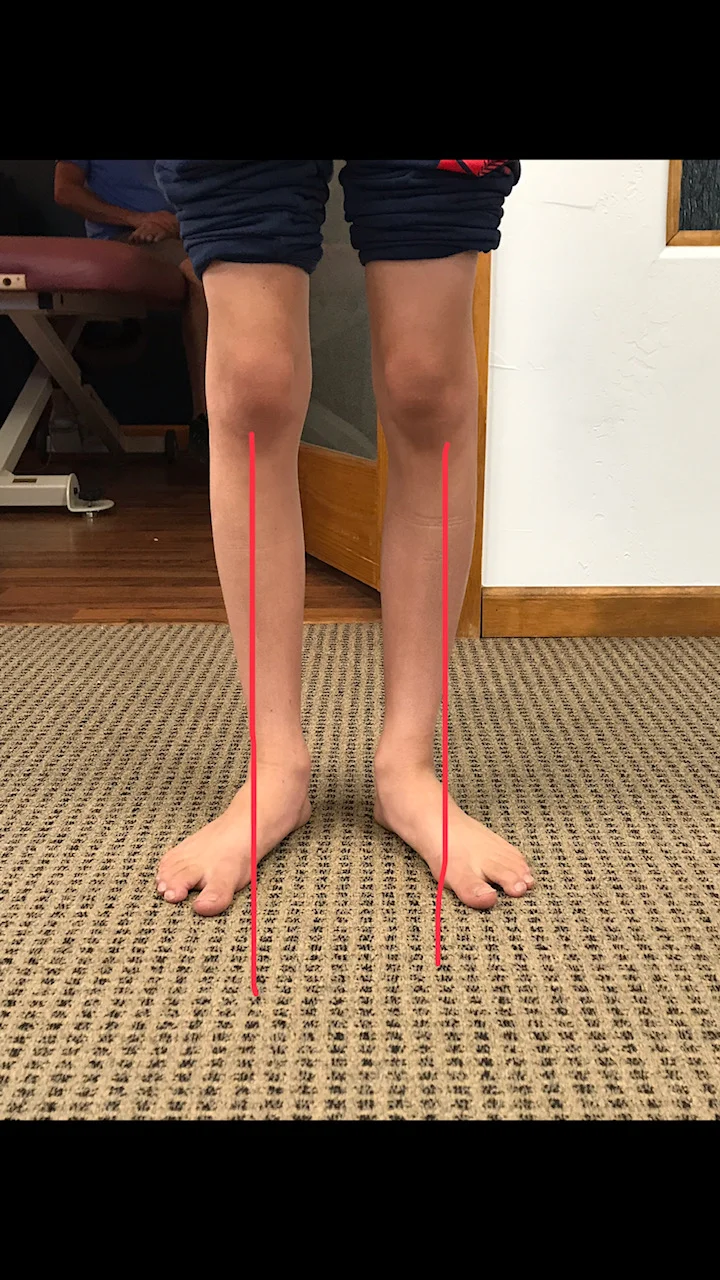
The patient DOES NOT have a leg length deficiency.
We remember that there are 3 systems that keep us upright in the gravitational plane:
1. vision
2. vestibular system
3. proprioceptive system
We also remember that as one of these systems become impaired, the others will usually increase their function to help maintain homeostasis. All these systems are known to decline in function with aging. So we have 3 systems breaking down simultaneously.
Did you also note the head forward posture, to move the center of gravity forward? How about the subtle head tilt to the right and “bobble” right and left? Motions which have to do with the head are functions of the vestibular system. He is attempting to increase the input to these areas (by exaggerating movements) to increase input.
How about the glasses? Presbyopia (hardening of the lens) makes it more difficult to focus. Movement (detected largely by rods in the eyes have a much higher density than cones, which are for visual acuity). By moving the head, he provides more input to the visual (and thus nervous system)
Amplified extremity movements provide greater input to the proprioceptive system (muscle spindles and golgi tendon organs (GTO’s), as well as joint mechanoreceptors).
Think of the cortical implications (and effects on the cerebellum, the queen of motor activity and important component for learning). You are witnessing the cognitive effects of aging playing out on the ability to ambulate and its effect on gait.
So what do we do?
Improve quality of joint motion, whether that is mobilization or manual methods to improve motion where motion is lost. Perhaps acupuncture to help establish homeostasis and improve muscular function. There are many options.
Postural advice and exercises
Core work
Proprioceptive exercises (like head repositioning accuracy, heel to toe and heel to shin)
Gait retraining
You get the idea. Providing some of that increased input for him and helping the system to better process the information will be the key to improving his function and helping to counteract and maybe slow the effects of aging on the locomotor system.
We are the Gait Guys; giving you the info so we can all make a difference, every day
We will be talking about some principals of proprioceptive rehabilitation along with 2 cases of neurological disorders Wednesday evening for our "3rd Wednesdays" talk on online.com: Biomechanics 321. 5 PST, 6MST, 7CST, 8EST
Special thanks to RM, who allowed us to use this video for this discussion.